Download
1 / 44
460 likes | 1.12k Vues
COMPATIBILITY TESTING. Dr. MOHAMMED H SAIEM ALDAHR BLOOD BANK 3 RD MEDICAL TECHNOLOGY. COMPATIBILITY TESTING. Out line Collection and Preparation of Samples Collecting Patient Samples Donor Samples Selection of Appropriate Donor Units Testing of the donor sample

E N D
COMPATIBILITY TESTING Dr. MOHAMMED H SAIEM ALDAHR BLOOD BANK 3RD MEDICAL TECHNOLOGY drmsaiem
COMPATIBILITY TESTING Out line • Collection and Preparation of Samples • Collecting Patient Samples • Donor Samples • Selection of Appropriate Donor Units • Testing of the donor sample • Testing of the patient sample • Cross-match • Summary of Pre-transfusion Testing drmsaiem
COMPATIBILITY TESTING • As the knowledge of new blood group system increased, so did the search for more sensitive pre-transfusion compatibility testing methods. Pioneer blood bankers mixed the patient’s serum and the donor’s red cells and observed for direct red blood cells lysis, agglutination, or both. This became known as the major cross-match test. • The term compatibilitytest and cross-match are some times used interchangeably, they should be clearly differentiated. drmsaiem
COMPATIBILITY TESTING • The cross-match became part of a series of pre-transfusion test known as compatibility testing. The compatibility test includes an ABO and Rh grouping performed on the donor and recipient samples, screening of the donor’s and patient’s sera for unexpected antibodies, and a cross-match. • The purpose of pre-transfusion or compatibility testing is to ensure the best possible results of a blood transfusion. • The transfused red cells will have an acceptable survival rate, and there will be no significant destruction of the recipient’s own red cells. drmsaiem
COMPATIBILITY TESTING • Collection and Preparation of Samples. Positive Patient Identification The major cause of transfusion associated fatalities have been clerical errors resulting in incorrect ABO grouping The most common cause of clerical errors and thus transfusion accidents is misidentification of the patient involved in the transfusion. Confusion in identification of the patient when the blood sample was drawn a mixed up samples during handling in the lab, and error in identification of the patient when the transfusion was given. drmsaiem
COMPATIBILITY TESTING • To prevent collection of samples from the wrong patient, the blood request form must be used to confirm the patient’s identity before phlebotomy is performed. The request form must state the intended recipient’s full name, and unique hospital identification number. Other information such as age and date of birth, address, sex, and name of requesting physician can be used to verify patient identity further but is not required on the form. drmsaiem
COMPATIBILITY TESTING • The patient’s wrist band identification must always be compared with the requisition form. • If the patient does not have a wristband or if the patient’s identity is unknown, some form of positive identification must be attached to the patient before collection of samples. drmsaiem
COMPATIBILITY TESTING • Collecting Patient Samples Hemolyzed samples can not be used for testing because hemolysis caused by activation of complement Serum or plasma may be used for pre-transfusion testing. Most blood bank technologist prefer serum because plasma may cause small fibrin clots to form which may difficult to distinguish from true agglutination. drmsaiem
COMPATIBILITY TESTING • When a specimen is received in the lab, a blood bank technologist must confirm that the information on the sample and requisition form agree. • All discrepancies must be resolved before the sample is accepted, and if any doubt exists, a new sample must be drawn. drmsaiem
COMPATIBILITY TESTING • Donor Samples. • Donor testing samples must be taken when the full donor unit is drawn. Depending on the method used for testing, clotted sample, anti-coagulated samples, or both, are obtained. Donor information and medical history card, the pilot samples for processing, and the collection bag must all be labeled with the same unique number code before starting the phlebotomy, and the numbers must be verified again immediately after filling. drmsaiem
COMPATIBILITY TESTING • Donor and recipient samples must be stored for a minimum of 7 days following transfusion. • The samples should be stoppered and refrigerated at 1-6°C, carefully labeled, and adequate in volume so that they can be re-evaluated if the patient experiences an adverse response to the transfusion. drmsaiem
Compatibility Testing Protocols. Selection of Appropriate Donor Units. In almost all cases, blood and blood components of the patient’s own ABO and Rh group should be selected for transfusion. When blood and blood components of the patient’s type are unavailable or when some other reason precludes their use, units selected must lack any Ag against which the patient has a significant Ab. drmsaiem
Selection of Appropriate Donor Units. • When transfusion of an ABO group different from the recipient must be given, packed red cells must be used rather than whole blood which contains plasma Abs that are incompatible with the patient’s red blood cells. • Group O packed red blood cells can be safely used for all patients, however, conservation of a limited supply of group O blood should dictate its use for patients of other AB types only in special circumstances. drmsaiem
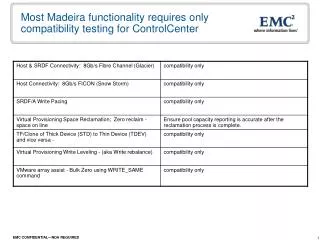
Selection of Appropriate Donor Units. • If ABO-specific blood is not available or is in less than adequate supply, alternative blood groups are chosen as summarized in the following table; Patient ‘s BGAlternative BG given as packed cells O NONE A O B O AB A, B, O only one of the three should be used for a given patient drmsaiem
Selection of Appropriate Donor Units. • Rh-negative blood can be given to Rh-positive patients, however, good inventory management again should conserve this limited resource for use in Rh-neg recipients. • If Rh-neg units is near expiration, the unit should be given rather than wasted. drmsaiem
Selection of Appropriate Donor Units. • Rh-pos blood should not be given to Rh-neg women of childbearing age. • Transfusion of Rh-neg male patients and female patients beyond menopause with Rh-pos blood is acceptable as long as no performed anti-D is demonstrable in the sera. drmsaiem
Compatibility Testing Protocols. Testing of the donor sample. • According to the Code of Federal Regulation (CFR) and the American Association of BB (AABB) standards, ABO and Rh grouping (including a test for weak D) and tests intended to prevent disease transmission must be performed on a sample of blood taken at the time of collection of the unit of blood from the donor. • A screening test for unexpected antibodies to red blood cell Ags is required by AABB standards on samples from donors revealing a history of prior transfusion or pregnancy. drmsaiem
Testing of the donor sample • The transfusing facility is required by AABB standards to confirm the ABO cell grouping on all units and Rh grouping on units labeled Rh-neg. • Tests for weak D (Du) are not required to be reported. The transfusion facility does not need to repeat any other testing procedure. drmsaiem
Testing of the patient sample. • A record of all results obtained in testing patient samples must be maintained. • Identification number should be assigned each time a patient is admitted for treatment. • Any discrepancies between previous and current results must be resolved before transfusion is initiated. • A new sample should be collected from the patient, if necessary to resolve the problem. • ABO and Rh grouping results should be included in the file. • Also, notations concerning unusual serologic reactions and the identity of unexpected Abs in the patient’s serum should be included. drmsaiem
Testing of the patient sample. • ABO and Rh grouping and Ab screening of the patient’s serum can be performed in advance of or at the same time as the cross-match. • If the patient has had a transfusion or has been pregnant within the last 3 months or if the history is unavailable or uncertain, the sample must be obtained from the patient within 3 days of scheduled transfusion. drmsaiem
Testing of the patient sample. ABO Grouping. • Determination of the patient’s correct ABO group is the most critical pre-transfusion serologic test. • If the cell and serum grouping results do not agree, additional testing must be conducted to resolve the discrepancy. • If the patient’s ABO group cannot be satisfactory determined and immediate transfusion is essential, group O packed red blood cells should be used. drmsaiem
Testing of the patient sample. Rh Grouping. • Rh grouping is performed using anti-D blood grouping serum. Tube or slide tests should be performed according to the manufacture’s directions for the reagent, which may or may not include the use of a suitable diluents control. • Control must be run in parallel with Rh grouping tests performed on patient’s samples, to avoid incorrect designation of Rh neg, patient as Rh positive. drmsaiem
Testing of the patient sample. • Direct antiglobulin test (DAT) should be performed on the patient’s red blood cells to determine whether uptake of autoantibody, (alloantibodies, if the patient’s has been recently transfused) is responsible for the positive control result. drmsaiem
Testing of the patient sample. • If the Rh group of the recipient can not be determined and transfusion is essential, Rh negative blood should be given. • The test for Du is unnecessary when testing transfusion recipients. Individuals typing as Rh neg in direct testing should receive Rh-neg blood and those typing as Rh pos in direct testing should receive Rh pos blood. • As Du are considered Rh pos and may receive Rh pos blood during transfusion. drmsaiem
Testing of the patient sample. Antibody Screening. • The patient’s serum or plasma must be tested for unexpected Abs. • The aim of the Ab screening test is to detect as many clinically significant Abs as possible. • Clinically significant Abs refers to Abs that are reactive at 37°C or in the DAT or both and are known to have caused a transfusion reaction or unacceptably short survival of the transfused red blood cells. drmsaiem
Testing of the patient sample. • Abs Regarded as always being potentially clinically significant ABO Rh Kell Duffy Kidd S s U • Abs that may sometime be clinically Significant Lea p Lua Lub Cartwright. • Abs that rarely, if ever, are clinically significant Leb Chido/Rodgers (Cha/Rha) York, Sd Xg& Bg drmsaiem
Testing of the patient sample. • Correct ABO grouping results are much more critical to transfusion safety than Ab screening. • Most Abs, other than anti-A and anti-B do not cause severe hemolytic transfusion reactions. Thus the vast majority of patients would not suffer grave consequences if transfused with blood from ABO group compatible donor without the benefit of Ab screening tests. drmsaiem
Testing of the patient sample. • Detection of unexpected Abs is important, however, for the selection of donor red blood cells that are likely to survive maximally in the patient circulation. • Weakly reactive Abs that are capable of reacting with their Ags at 37°C can cause decreased survival of transfused incompatible red cells. drmsaiem
Testing of the patient sample. • Because large numbers of Ab molecules are present in the patient’s circulation compared with the number of red cells in a unit of blood, incompatible donor cells are highly vulnerable to destruction by patient Abs. • Abs screening offers several advantages over direct cross-matched testing for detection of Abs; • 1- Testing is performed using selected group O red cells that are known to carry optimal representation of important blood group Ags. drmsaiem
Testing of the patient sample. • 2- Testing can be performed well in advance of the anticipated transfusion, allowing ample time for identification of unexpected Ab and location of suitable donor units lacking the corresponding Ag. • Methods used to detect Abs in patient’s sera must demonstrate all significant coating, hemolyzing, and agglutinating Abs active at 3 7°C. drmsaiem
Cross-match • The two main functions of the cross-match test can be cited as, I- It is a final check of ABO compatibility between donor and patient. 2- It may detect the presence of an Ab in the patient’s serum that will react with Ags on the donor RBCs but that was not detected in the Ab screening because the corresponding Ag was lacking from the screening cell. drmsaiem
Cross-match Major and Minor cross-match tests • Major cross-match test, consisting of mixing the patient’s serum with donor RBCs. • Minor cross-match test, consisting of mixing the donor’s plasma with patient’s RBCs • The minor cross-match test has been completely eliminated in most blood banks, because donor samples are screened beforehand for the more common Abs. drmsaiem
Cross-match Method for major cross-match tests. • Cross-match methods can be categorized by the test phase in which the procedure ends. • Immediate spin (IS) cross-match (Abbreviated Cross-match) • When no clinically significant Abs are detected nor are there previous record of such Abs, a serologic test to detect ABO incompatibility is sufficient. drmsaiem
Cross-match • In IS (the patient’s serum with donor cell are centrifuge immediately) absence of hemolysis or agglutination indicates compatibility. • False reaction may be seen in the presence of other IS reaction (auto -I). In patient with hyperimmune ABO Abs, when the procedure is not performed correctly (delayed in centrifugation or reading) when rouleauex is observed, or when infant’s specimens are tested. drmsaiem
Cross-match Antiglobulin Cross-match • The procedure begin in the same manner as the IS cross-match, continues to 37°C incubation and finishes with AHG test. drmsaiem
SUMMARYPRE TRANSFUSION TESTING • Is to provide safe, compatible blood for transfusion to each individual patient. The steps necessary for safe transfusion are: • 1. Accurate ABO and Rh typing of the patient. • 2. Accurate ABO and Rh typing of the donor. • 3. Screening tests for antibodies in the donors and patients serum. • 4. In the presence of patient antibodies, selection of appropriate units for each patient. • 5. Compatibility Testing - (Major) • 6. Accurate completion of paperwork and labels drmsaiem
PRE TRANSFUSION TESTING Compatibility Testing Each compatibility test is a unique experiment in which an unknown (patient) serum and (donor) red cells are tested for the detection of unexpected antibodies which are directed against antigens found on the cells. Negative results indicate compatibility. This is one of the most important tests performed by a transfusion service. drmsaiem
PRE TRANSFUSION TESTING • The purposes of compatibility testing are: • 1. To detect irregular antibodies in the recipient serum that are directed against the donor’s cells. • 2. To detect errors in ABO grouping. • 3. To detect errors in labeling, recording, or identifying donor’s or recipient’s samples. drmsaiem
PRE TRANSFUSION TESTING Compatibility testing does not: • 1. Ensure normal survival of donor red cells. • Prove that donor and or recipient serum is free of antibodies. Prevent immunization of the recipient. • Detect ALL ABO typing errors. • Detect errors in Rh typing of either recipient or donor unless the recipient’s serum contains an Rh antibody. • Detect ALL error of identification. • Pre-transfusion testing of the recipient must include an ABO and Rh typing, antibody screen, and a cross-match with all donor units. drmsaiem
Patient red cell with –D Ag. drmsaiem
If Rh –ve do drmsaiem