Download
1 / 52
600 likes | 3.86k Vues
Hyponatremia Anthony R Mato, MD Remember the basics of the body’s fluid compartments. TBW = WEIGHT x .5 (women) or .6 (men) TBW x 1/3 = ECF TBW x 2/3 = ICF ECF x 2/3 = Interstitial compartment ECF x 1/4 = Intravascular compartment

E N D
Hyponatremia Anthony R Mato, MD
Remember the basics of the body’s fluid compartments. • TBW = WEIGHT x .5 (women) or .6 (men) • TBW x 1/3 = ECF • TBW x 2/3 = ICF • ECF x 2/3 = Interstitial compartment • ECF x 1/4 = Intravascular compartment • Water will move freely to balance osmolalities: Therefore all compartments have equal osmolalities. • Sodium is the major extracellular cation.
King Sodium : Rules the ECFV • The total amount of Na in the ECF is the main determinant of the size of the ECFV. • If ECF Na increases so will the ECFV. • The edematous states: CHF, liver cirrhosis, and nephrotic syndrome are examples of increased total body Na in the extracellular compartment causing volume overload.
ECFV overload results from too much sodium in the ECF compartment. ECFV depletion results from too little sodium in the ECF compartment.
The Axis of Sodium • The kidney controls the size of the ECFV by controlling Na excretion. • Kidney is programmed to keep the ECFV within an acceptable range. The kidney will use 3 systems to regulate ECFV (afferent sensory arm to sense ECFV and efferent arm to effect change). • Renin – AT II – Aldosterone axis • ANP system • Sympathetic nervous system
It’s NOT IMPORTANT TO MEMORIZE THE PATHWAYS. IMPORTANT TO KNOW : that when ECFV increases mechanisms are triggered to excrete Na as the response. When ECFV decreases mechanisms are triggered to retain Na as the response.
NOTE THAT WE HAVE NOT YET MENTIONED THE CLINICAL MEASURE OF SODIUM CONCENTRATION. [Na] is a measure of Na relative to water. It tells you NOTHING about the total body sodium. Abnormalities in the Na concentration tell us that there are abnormalities in the amount of WATER in the ECF compartment.
Osmolality vs. Tonicity • Osmolality: total solute concentration in a fluid compartment. • Tonicity: the combined ability of solutes to produce a osmotic driving force that causes water to move from one compartment to another. • Solutes that are capable of moving water are called “effective osmoles”. • These are solutes that are unable to cross from the extracellular to the intracellular compartment: sodium, glucose, mannitol, sorbitol. NOT UREA. • The control of tonicity will determine the normal state of cellular hydration and cell size. This is of particular concern in the case of brain cells.
Osmolality • Osmolality = Osmoles/kg of water • 2(Na+) + Glucose/18 + BUN/2.8 • Normal is 285-295
To regulate water excretion and keep the tonicity (Na concentration) of ECFV constant there must be: • Adequate GFR. • Delivery of GF to the concentrating and diluting segments of the loop of Henle and distal nephron. • Intact tubular concentrating and diluting mechanisms, • Appropriate turning on/off of ADH. • ADH responsiveness of the kidney.
ALL OF THE CLINICAL DISORDERS PRODUCING HYPER AND HYPONATREMIA MAY BE UNDERSTOOD AND REMEMBERED BASED ON ABNORMALITIES OF THESE MECHANISMS.
A Note on Diuretics • Both loop and thiazide diuretics block the reabsorption of Na and can therefore can lead to a decrease in the size of the ECFV. • They DIFFER in that loops produce a balanced loss of Na and Water therefore Na concentration is usually undisturbed. • Thiazide causes an unbalanced loss of Na and Water – such that more Na is lost relative to water causing hyponatremia.
The Body Has Simple Goals Goals of the body • Maintain Na concentration within a narrow range. • Maintain ECFV within an acceptable range.
Volume Status is a Na Problem • IN CLINICAL PRACTICE, IT IS MOST USEFUL TO CONSIDER THAT CASES OF ABNORMAL ECFV SIZE ARE DUE TO PROBLEMS WITH THE CONTROL MECHANISMS regulating TOTAL BODY SODIUM. • Ask yourself, how might the Na mechanisms be impaired. • Volume overload can be viewed as being total body Na overloaded. • Volume depletion can be viewed as having too little total body body Na.
[Sodium] is a water problem. • IN CLINICAL PRACTICE, IT IS MOST USEFUL TO CONSIDER THAT CASES OF ABNORMAL ECF SODIUM CONCENTRATION ARE DUE TO PROBLEMS WITH THE WATER CONTROL MECHANISMS. • Ask yourself, how might water controlling mechanisms be impaired. • This is where the diagnosis and treatment must focus.
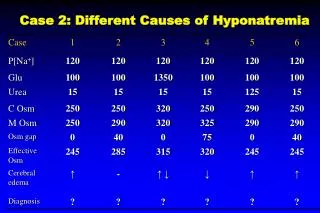
ATTACK VOLUME AND SODIUM CONCENTRATION AS TWO SEPARATE PROBLEMS. THIS TABLE WILL HELP BREAK IT DOWN.
Causes of Hyponatremia: most cases will by the hypotonic, hypoosmolar state. • Pseudohyponatremia: [Na] is low, but serum osm is normal. This value is an artifact due to the accumulation of other plasma constituents in plasma: hypertriglyceridemia, hyperproteinemia (MM). • Here measured osm are normal but the calculated osm will be low (low Na). • The patient will be asymptomatic since the tonicity is normal. • This is rare now since the Na electrode method is used to measure serum [Na].
Causes of Hyponatremia: most cases will by the hypotonic, hypoosmolar state. • Hyponatremia with hypertonicity: [Na] is low since water will flow into the ECF compartment as a result of hyperglycemia for example. • The calculated and measured osm will be elevated in that case. Na will decrease by approx 1.6 meq/dL for every 100 mg/dl increase in glucose above 100. • In the case of mannitol the measured osm will be high but the calculated osm will be low.
Hyponatremia with hypotonicity: impaired renal water excretion in the setting of continued water intake. THE REASON WHY THE KIDNEY CAN NOT CONCENTRATE THE URINE IS THE KEY TO DIAGNOSING THE CAUSE OF HYPONATREMIA.
Use your physiology to figure it out. March down the nephron. • Impaired GFR: if one cannot filter a water load then one cannot excrete a water load. At GFR of < 20% we start to have problems with water handling. • ECFV depletion : gastric losses with water depletion. Proximal tubule is the culprit: solvent drag. • Edematous states: These people have abnormal retention of Na and water. CHF, liver, nephrotic disease.
Use your physiology to figure it out. March down the nephron. • Thiazide diuretics: block the kidney’s ability to produce a dilute urine. • SIADH: pituitary release, ectopic production, ADH-like meds, potentiation effects of meds on ADH action at the renal tubule. • Endocrine: Hypothyroidism and Hypoadrenalism. • You can’t make a concentrated urine if you do not have an adequate solute intake. These patients are usually elderly and have a decreased osm excretion. Tea and Toast. • Beer drinkers also take in large amounts of fluids with a relatively low solute load.
Treatment • The rapidity of the development of hyponatremia is more important than the actual value of the serum sodium concentration. • In the chronic / slow setting the cells have time to transport intracellular solutes to the extracellular space to account for the hypotonicity of the extracellular space. • If this is corrected rapidly osmotic demyelination syndrome can occur. • The most severe form of ODS will be quadriplegia (the locked in syndrome).
Chronic Hyponatremia • Keep in mind that to develop progressive hyponatremia you need an impairment of water excretion as well as continued water intake. (ESRD patient). • Before you diagnose a specific etiology you can always restrict free water intake to 800 cc / day as a temporizing / stabilizing measure
Volume overloaded states • Water restriction is also the appropriate treatment for hyponatremia. • This will deal with the water excretion problem and loop diuretics will deal with the hypervolemia state (sodium overload problem). • Thiazides can acutely worsen the situation. • IF THERE IS NO HYPONATREMIA IN THE VOLUME OVERLOAED STATE THEN THERE IS NO NEED TO RESTRICT WATER. • IF EDEMA IS THE SOLE PROBLEM THEN IT IS A PROBLEM OF SODIUM EXCRETION – AND YOU WILL NEED TO INCREASE SODIUM EXCRETION AND RESTRICT SODIUM INTAKE.
ECFV Depletion: The Vomiting Patient • In ECFV depletion you have a water and sodium problem. • Urine sodium will be low. • *Urine Na will also be low in the hypervolemic states as well. • These people will usually respond to NS. • Physiologically the culprit is the proximal tubule.
SIADH Treatment • Water restriction. • NaCl tablets (as a solute load) • Demclocycline. • ADH receptor antagonists (The future?) • Find the underlying cause of the hyper ADH state.
Acute / Symptomatic Hyponatremia • Correct Na no faster than 1 meq / L per hour until achieving a 6-8 meq / L increase, then .5 meq / L / hour or less. • Permit no more than 10-12 meq/ L increase in Na over 1st 24 hours. • Slow or stop infusions when symptoms improve. • The goal is not correct the serum sodium, but to correct the cerebral edema.
How to use 3% Saline. • Sodium deficit : Na desired – Na measured x TBW • 513 meq Na in 1 L of 3% saline: Sodium deficit / 513 will give you the volume to infuse. • Set the rate. • This should be done with the guidance of renal medicine. This should be done in an ICU setting. • Once we have treated the symptoms we can stop this dangerous drug and start more conservative measures as treatment.
Adheesh 23 yr old male develops watery diarrhea. He comes to your ER lightheaded and orthostatic. He has dry MM and tachycardia. Neuro exam is normal and he is alert. Labs: Na 129, K 3, HCO3 20, BUN 20, Cr 1, Glucose 75, Urine Na 5, Urine osm 520.
Adheesh • What is serum OSM? • What is volume status? • Is the volume loss renal / extra renal? • What is the cause of the hyponatremia? • How would you treat this patient?
“I ran out of insulin” case 72 yr old woman with DM presents to ER with polyuria and polydipsia x 5 days. PE is normal. Labs: Na 129, K 4.2, Cl 89, HC)3 24, BUN 5, Cr.08, Glucose 780. What is the osm? Why is he hyponatremic? What is the corrected Na? What is the treatment?
Unresponsive: A Na emergency 38 yr old woman with Hep C is brought to ED unresponsive. She is obtunded with elevated JVP, rales b/l, massive ascites, and 2 + edema. Labs: Na 112, K 4.1, Cl 89, HCO3 24, BUN 32, Cr .7, Glucose 90, Urine Na 2, Urine OSM 800. What is the osm? What is the volume status? Why is she hyponatremic? What is the treatment(s)?
Case 1 You are called as a curbside consult for an outpatient hyponatremia case. Serum Na is 120. Pt is asymptomatic. Other data: Cl 80, K 4.5, HCO3 24, BUN 14, glucose 90. What further questions do you ask?
Case 2 A 50 yr old male with h/o hyperlipidemia has the following labs: Na 125, M-Osm 270, TGs 1000, total protein 8.5. The blood is lipemic. Is this a case of pseudohyponatremia?
Case 3 Mr. T has 3 days of N/V, polyuria and polydipsia. Exam: poor turgor and orthostatic. Labs: glucose 360, Na 120, BUN 28. M-OSM 270. What is the cause of this hyponatremia? What will Na be once glucose is corrected to 100?
Case 4 Mrs. NA has polyuria, polydipsia, and delta MS. Exam shows poor turgor and orthostasis. Labs: glucose 2100, Na 130, BUN 40. M-OSM = 395. What is the cause of the hyponatremia? What will Na be once glucose is corrected? What fluid should you use?
Case 5 Mr. JD comes to the ER staggering and smelling foul. Na is 140, glucose 180, and BUN 28. M-OSM = 330. What is your diagnosis? How could you confirm it using the above lab data?
Case 6 RR has a classic exam in addition to his new onset edema after eating some chips. He has elevated JVP, crackles, S3. CXR shows b/l pulmonary edema. Labs Na 125, urine Na 5, M OSM 270. Why is serum Na low? How would you treat this?
Case 7 RR return to clinic in florid CHF. This time his Na is 138. What treatments would you now offer him?
Case 8 Jenny a 46 yr old female presents with N/V and abdominal pain. MM are dry, skin has poor turgor, and she is orthostatic. She notes a h/o PUD. Labs: Na 125, U Na 5, M OSM 270. What is happening? What therapy do you implement?
Case 9 72 yr old male who is a heavy smoker presents with cough and hemoptysis. His physical exam is completely normal in terms of volume status. CXR reveals a 6 cm left sided chest mass. Labs: Na 125, K 4.2, Cr 1.1, M OSM 270, Urine Na is 45. He takes no meds. TSH and am cortisol are normal. What is causing the hyponatremia?