Download
1 / 42
430 likes | 1.04k Vues
Racial Disparities and Breast Cancer in Nevada. 2007 First Lady’s Conference on Women’s Health Issues. Norma Goode RN BSN Breast Health Educator/Navigator Nevada Cancer Institute.

E N D
Racial Disparities and Breast Cancer in Nevada 2007 First Lady’s Conference on Women’s Health Issues Norma Goode RN BSN Breast Health Educator/Navigator Nevada Cancer Institute
“Communities of color suffer disproportionately from diabetes, heart disease, HIV/AIDS, cancer, stroke and infant mortality. Eliminating these and other health disparities is a priority of HHS.” -- Former DHHS Secretary Tommy Thompson “We need to focus on the uninsured and those who suffer from health care disparities that we so inadequately addressed in the past”. --Sen Bill Frist (R-Tenn)Former Senate Majority Leader on his priorities for the 108th congress
Objectives • Identify racial disparities and barriers to breast cancer • Describe cultural differences and the dynamics between the races • Discuss the genetics in African American women that make cancer cells more aggressive
Disparities Defined “Differences in the incidence, prevalence, mortality and burden of diseases and other adverse health conditions that exist among specific population groups in the United States”. – National Institutes of Health, 1999 “A population is a health disparity population if there is significant disparity in the overall rate of disease incidence, prevalence, morbidity, mortality or survival rates in the population as compared to the health status of the general population”. – Minority Health and Health Disparities Research and Education Act, United States Public Law 106-525 (2000)
Health of the United States • In 1984: Health, United States 1983 was sent to congress. Findings in the report revealed significant progress: -Americans were living longer -infant mortality had continued to decline -overall improvement in American health But, there existed a continuing disparity in the burden of death and illness experienced by Blacks and other minority Americans as compared with our nations population as a whole Department of Health and Human Services, Task Force on Black and Minority Health, 1985
Racial Disparities- IOM* Findings • 1-1:Racial and ethnic disparities in healthcare exist • 2-1:They occur in the context of broader historic and contemporary social and economic inequality *Institute of Medicine, Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care, 2002
Racial Disparities- IOM Findings • 3-1: Many sources contribute to racial and ethnic disparities in healthcare • 4-1: Bias, stereotyping, prejudice, and clinical uncertainty also contribute to racial and ethnic disparities in healthcare.
Racial Disparities- IOM Findings • 4-2: Minority patient refusal rates are small and don’t fully explain healthcare disparities • Mistrust? • Negative experience in the clinical encounter? • Perception that HCP is not invested in their care?
National Healthcare Disparities Report • An annual report released by the Agency for Healthcare Research and Quality (AHRQ) • Provides a comprehensive national overview of disparities in health care among racial, ethnic, and socioeconomic groups • Tracks the success of interventions to reduce disparities uses measures of quality to determine if nation is making progress toward eliminating health care disparities
National Healthcare Disparities Report, 2006 4 key themes: • Disparities remain prevalent • Some disparities are diminishing, others are increasing • Opportunities for improvement remain • Information about disparities is improving, but gaps still exist
Racial Disparities in Breast Cancer
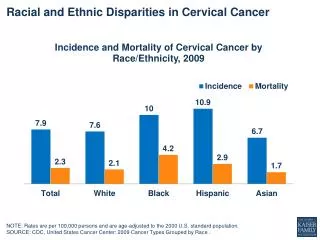
Racial Disparities in Breast Cancer • White women are more likely to develop breast cancer than African American women. But, African American women are more likely to die of this cancer (DHHS, Office of Minority Health, May 2005). • African-Americans have the highest mortality rates and the lowest survival rates². - dx later and at more advanced stages - Black women consistently develop larger primary tumors, high rate of spread to lymph nodes, more distant metastatic disease³
Breast Cancer in Nevada
Racial and Ethnic Breast Cancer Rates- Nevada American Cancer Society, 2005 Healthy People Nevada 2010 Healthy People Nevada 2010
Barriers to Treatment* • Health care system -lack of health insurance • Barriers within the system • Provider issues: -patient-provider communication -patient-provider relationship -cultural competency -and health information • Utilization of care- focus on receipt of health care (i.e. routine, acute, chronic care) *National Healthcare Disparities Report, 2003
Cultural Differences and Dynamics • 85 to 90% of cancer incidence is attributable to lifestyle choices, such as diet, life habits such as smoking, and environmental factors. Culture is the single force most influential on lifestyles. (Kagawa-Singer, M., (2000). A socio-cultural perspective on cancer control issues for asian americans,8:12-17) • The variable “race” subsumes potential cultural differences, such as diet and lifestyle; economic factors such as access to care; and educational factors such as knowledge about guidelines for early detection and treatment (http://cancercontrol.cancer.gov/womenofcolor/african.html) • We need to understand the potential contributions of socio-cultural factors to cancer control.
Cultural Differences and Dynamics- minority groups African Americans -past treatment in most US history -24% below poverty line (ACS, 2007-2008) -high teen pregnancy rates -church/community http://cancercontrol.cancer.gov/womenofcolor/african.html
Cultural Differences and Dynamics- minority groups • Hispanics -fastest growing population -Mexican-Americans represent ~60% -low income/poverty/education -reading not the common form of communication -effects of acculturation -strong social support, familism, faith -fatalistic attitude (http://dccps.nci.nih.gov/womenofcolor/mexican.html)
Cultural Differences and Dynamics- minority groups • Asian American -modesty -language -fears -lack of preventive measures -fatalistic attitude due to “karma” -alternative medicine -one of the fastest growing minority (http://dccps.nci.nih.gov/womenofcolor/asian.html)
Cultural Differences and Dynamics- minority groups • American Indian -taboos about discussing cancer -reluctance to “look for illness” -no word for cancer -fatalistic attitude -cancer survivors are not visible http://dccps.nci.nih.gov/womenofcolor/indian.html
Cultural Competency “Culture and linguistic competence is a set of congruent behaviors, attitudes, and policies that come together in a system, agency, or among professionals that enables the effective work in cross-cultural situations”. “Culture refers to integrated patterns of human behavior that include the language, thoughts, communications, actions, customs, beliefs, values, and institutions of racial, ethnic, religious, or social groups”. “Competence implies having the capacity to function effectively as an individual and an organization within the context of cultural beliefs, behaviors, and needs presented by consumers and their communities”. Based on Cross, T., Bazron, B.,, Dennis, K., & Isaacs, M. (1989). Towards a Culturally Competent System of Care, Volume 1. Washington DC: Georgetown University Child Development Center, CASSP Technical Assistance Center.
Cultural Competency * • Providing culturally and linguistically appropriate services (CLAS) to patients has the potential to improve access to care, quality of care, and, ultimately health outcomes • National standards were issued by DHHS, Office of Minority Health, to ensure that all people entering the health care system receive equitable and effective treatment in a culturally and linguistically appropriate manner *US Dept of Health and Human Services, Office of Minority Health, National Standards for Culturally and Linguistically Appropriate Services in Healthcare, Final Report, 2001
CLAS Standards- culturally competent care • Health care organizations (HCO) should ensure patients receive care that is compatible with health beliefs and practices and preferred language • Recruit, retain and promote diverse staff and leadership • Ensure staff receive ongoing education and training
CLAS Standards-Language access services 4. Offer and provide language assistance service 5. Provide verbal and written notification of language services 6. Assure competence of language assistance provided 7. Make available patient-related materials and post-signage in languages commonly encountered
CLAS Standards- organizational supports 8. Develop, implement, promote plan that oversees provisions of culturally and linguistically services 9. Conduct ongoing assessments 10. Document data on patient’s race, ethnicity and spoken language in health record
CLAS Standards 11. Maintain a current demographic, cultural and epidemiological profile of the community 12. Develop partnerships with community to design and implement CLAS activities 13. Ensure conflict and grievance resolution are culturally and linguistically sensitive 14. Provide public information about CLAS implementation progress
African American Women and Breast Cancer • More aggressive tumors-prevalence of basal-type breast cancer, 2.1 times greater risk than others (NCI Cancer Bulletin , vol.3/no. 24, June 13, 2006) • Higher rate of estrogen-receptor (ER) negativity • Tumors tend to be less differentiated • Higher proliferative fraction • Worse prognosis overall; worse prognosis within each stage; present with more advanced disease • More likely to be younger at diagnosis Elledge, RM, Clark, GM, Chamness, GC, Osborne, CK (1994). Tumor Biologic Factors and Breast Cancer Prognosis Among White, Hispanic, and Black Women in the United States. Journal of the National Cancer Institute, 86: 705-712
Summary • Racial disparities exist • Efforts to reduce barriers to treatment • Importance of cultural competency/sensitivity • Addressing the needs of minority populations
References • Department of Health and Human Services, Office of Minority Health. (2005). Breast Cancer: A resource guide for minority women. Available from http://www.omhrc.gov/assets/pdf/checked/bcrg2005.pdf. • Smith-Bindman, R., Miglioretti, D.L., Lurie, N., Abraham, L., Barbash, R.B., Strzelczyk, J., Dignan, M., Barlow, W.E., Beasley, C.M. and Kerlikowske, K. (2006). Does utilization of screening mammography explain racial and ethnic differences in breast cancer? Annals of Internal Medicine, 144: 541-553. • Underwood, S.M.(2003). Reducing the burden of cancer borne by african-americans: If not now, when?. Cancer Epidemiology,Biomarkers & Prevention,12: 270s-276s. • Merkin, S.S., Stevenson, L. & Powe, N. (2002). Geographic socioeconomic status, race, and advanced-stage breast cancer in New York City. American Journal of Public Health,92: 64-70. • Department of Health and Human Services, Agency for Healthcare Research and Quality. (2005). National Healthcare Disparities Report. Available from http://www.ahrq.gov/qual/nhdr05/nhdr05.pdf • Carey, Lisa A., et al. (2006). Race, breast cancer subtypes, and survival in south carolina breast cancer study. JAMA, 295: 2492-2502.