Download
1 / 34
390 likes | 1.22k Vues
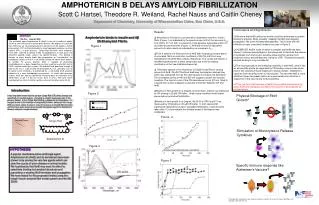
AMPHOTERICIN B NEPHROTOXICITY . GILBERT DERAY PARIS , FRANCE. * Amphotericin B (AmB) remains the most effective drug in treating systemic fungal infections. * Amphotericin B can produce a wide variety of acute and chronic side effects, the most important of which is nephrotoxicity .

E N D
AMPHOTERICIN B NEPHROTOXICITY GILBERT DERAY PARIS , FRANCE
*Amphotericin B (AmB) remains the most effective drug in treating systemic fungal infections *Amphotericin B can produce a wide variety of acute and chronic side effects, the most important of which is nephrotoxicity
INCIDENCE OF AMPHOTERICIN B NEPHROTOXICITY Authors Rate of nephrotoxicity 1998 White 64 % 1999 Walsh 49 % 1999 Wingard 53 %
RATE AND SEVERITY OF NEPHROTOXICITY AND HEMODIALYSIS IN PATIENTS TREATED WITH AMPHOTERICIN Creatinine values Dialysis required (% patients) (% patients) Doubled Increased to > 2.5 mg/dl 53 % 29 % 15 % Wingard et al, J Clin Inf Dis, 1999
PHARMACOECONOMICS OF HOSPITAL COSTS ACCORDING TO AMPHOTERICIN B RENAL TOXICITY Greenberg et al ,ICAAC,2000
THE EFFECTS OF ACUTE RENAL FAILURE ON MORTALITY Odds ratio of dying = 3.09 80 76 % Mortality (%patients) * 70 57 % * p < 0.05 vs NO 60 50 40 0 Hemodialysis Wingard JR, Clin Infect Dis, 1999
AMPHOTERICIN B NEPHROTOXICITY IS * Frequent * Severe * Associated with an increase in hospital costs * Associated with an increase in the risk of death Therefore we must If possible, prevent Amphotericin B nephrotoxicity.
Prevention of Amphotericin B nephrotoxicity * Intralipid * Risk factors * Early detection of renal toxicity * New formulations
AMPHOTERICIN B AND INTRALIPID * We lower the price but... * Do we lower the renal toxicity ? *And even so should we do it ?
PROSPECTIVE TRIALS COMPARING RENAL TOXICITY OF AMPHOTERICIN B IN EITHER GLUCOSE OR INTRALIPID Authors Patients Less nephrotoxicity with intralipid Moreau 1992 Haematological YES malignancies Caillot 1994 Haematological YES malignancies Sorkine 1996 ICU critical ill patients YES Schöffski 1998 Neutropenic patients NO Nucci 1999 Cancer NO
THE USE OF LIPID EMULSION WITH AMPHOTERICIN B Benefit ? Risks * Price * Effect on amphotericin B * Lower antimycotic nephrotoxicity ? activity * Cholestasis * Thrombocytopenia * Hepatic function abnormalities * Pulmonary toxicity we should NOT !!
Prevention of Amphotericin B nephrotoxicity * Intralipid * Risk factors * Early detection of renal toxicity * New formulations
RISK FACTORS FOR AMPHOTERICIN B NEPHROTOXICITY * Use of diuretics * Abnormal baseline renal function * Cumulative dose of Amphotericin B * Concomitant nephrotoxic drugs (cyclosporin,FK506,aminoglycosides...) * Dehydration * Patient category
AMPHOTERICIN B AND DIURETICS * There is no clinical evidence that diuretics prevent Amphotericin B nephrotoxicity. * Mannitol and Furosemide will aggravate hypokalemia and hypomagnesemia. * Diuretics are a risk factor for amphotericin B nephrotoxicity. * I do not recommend their use in this indication.
HYDRATION AND AMPHOTERICIN B *Dehydration is a key factor for the renal tolerance of all potential nephrotoxic drugs, *All patients should received 1 to 2 liters of isotonic saline prior to each amphotericin B infusion
RATE OF NEPHROTOXICITY AND HEMODIALYSIS IN 4 PATIENTS GROUPS Patients groups Nephrotoxicity Dialysis (CR x 2)(%) required (%) Allogenic BMT 61 20 Autologous BMT 80 19 SOT 35 18 Non Transplantation 54 7 Wingard JR, Clin Inf Dis, 1999
Prevention of Amphotericin B nephrotoxicity * Intralipid * Risk factors * Early detection of renal toxicity * New formulations
TUBULAR DYSFUNCTION INDUCEDBY AMPHOTERICIN B Incidence HypoK+ 25 - 75 % HypoMg 30 - 75 % Renal tubular acidosis 50-100 % Renal concentrating defects (polyuria) 50- 100 % * Usually before renal insufficiency * After 7 to 14 days of treatment * Dose-dependant response
AZOTEMIA *Is caracterized by a decrease in creatinine clearance and an increase in serum creatinine *Is preceded by tubular dysfunction *May be irreversible with large cumulative doses * Is underestimated with serum creatinine assessment
WHAT CHANGE IN SERUM CREATININE SHOULD BE CONSIDERED AS SIGNIFICANT ? • A 25% rise in serum creatinine level may appear to be small but actually represents a substantial fall in GFR -perhaps as much as a 50% reduction because of the exponential rise in serum creatinine level with declining renal function , • In addition, renal function and muscle mass decline more or less in parallel with advancing age or severe disease, so that the little old lady and your very sick patients with a mild increase in serum creatinine have a GFR only about 30% of that of a young healthy adult
EARLY DETECTION OF AMPHOTERICIN B NEPHROTOXICITY • Tubular dysfunction: hypokalaemia; hypomagnesemia; polyuria; tubular acidosis . And \ or • Renal insufficiency: a 25% rise in serum creatinine . Stop the drug...
Prevention of Amphotericin B nephrotoxicity * Intralipid * Risk factors * Early detection of renal toxicity * New formulations
Randomized, double blind clinical trial of Amphotericin B colloidal dispersion vs amphotericin B in the empirical treatment of fever and neutropenia. White et al. Clin Inf Dis, 1998. * 213 neutropenic patients * Hematologic malignancy or marrow transplantation * Treatment ABCD (4 mg/kg/d) vs conventional amphotericin B (0.8 mg/kg/d)
ABCD vs AMPHO B :RENAL INSUFFICIENCY % of patients with serum creatinine > 2 times baseline * * p < 0.05 vs ABCD ABCD Ampho B White M et al, Clin Inf Dis, 1998
ABLC for cryptococcal meningitis in AIDS patients Sharkey et al, CID, 1996 ; 22 : 315-321 * 55 AIDS patients * Cryptococcal meningitis * Treatments - Amphotericin B : 1 mg/kg/day - Abelcet® : 5 mg/kg/day 2.5 mg/kg/day 1.2 mg/kg/day
Comparative nephrotoxicity of Abelcet® and conventional Amphotericin B Ampho B Abelcet ® (5 mg/kg/day) Doubling in SCR 53 % 50 % HypoK+ 24 % 24 % HypoMg 24 % 24 % Sharkey et al, CID, 1996 ; 22 : 314-321 Luke R et al, Am J Kidney Dis, 1998 ; 31 : 780-785
Liposomal amphotericin B for empirical therapy in patients with persistent fever and neutropenia Walsh et al, N Engl J Med, 1999 * Double blind randomized study (n = 683) * Persistent fever and neutropenia (cancer, lymphoma, bone marrow transplantation) * Treatments - Ampho B : 0.6 mg/kg/day or - Ambisome : 3.0 mg/kg/day
AMBISOME® vs AMPHO B :RENAL INSUFFICIENCY % of patients with serum creatinine > 2 times baseline * p < 0.05 vs Ampho B * AmBisome® Ampho B Walsh et al, N Engl J Med, 1999
AMBISOME® vs AMPHO BHYPOKALEMIA (K+ < 2.5 mEq/l) % of patients with serum K+ < 2.5 mEq/l * * p < 0.05 vs Ampho Ambisome® Ampho B Walsh et al, N Engl J Med, 1999
A randomized double blind comparative trial evaluating the safety of Ambisome® versus Abelcet® in the empirical treatment of febrile neutropenia. Wingard et al, 9th focus on fungal infections, 1999 * Double blind randomized study (n = 250) * Neutropenic patients with unresolved fever * Treatments - Abelcet® : 5 mg/kg/day - Ambisome® : 3 mg/kg/day or 5 mg/kg/day
AMBISOME VS ABELCET:RENAL INSUFFICIENCY % patients with serum creatinine > 2 times baseline * * * p < 0.05 vs Abelcet ® Wingard et al, 9th focus on fungal infections, 1999
AMBISOME VS ABELCET:RENAL INSUFFICIENCY * % patients * 2 x baseline serum creatinine 1.5 x baseline serum creatinine * p < 0.05 vs Ambisome ® Wingard et al, 9th focus on fungal infections, 1999
CONCLUSIONS * Amphotericin B nephrotoxicity remains frequent and severe * Amphotericin B-induced acute renal failure is not a benign complication : -It increases hospital costs -It increases patient mortality
CONCLUSIONS The prevention of Amphotericin B nephrotoxicity rely on : *The detection and if possible the suppression of risk factors, *The use of liposomal formulation of Amphotericin B : (at least) - in high risk patients, - in patients with Amphotericin B nephrotoxicity.