Download
1 / 28
290 likes | 835 Vues
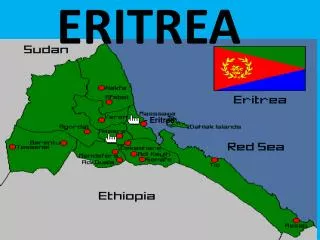
Effectiveness of malaria control in Eritrea, 1996 to 2003. Patricia M Graves June 6, 2008 IRI. Eritrea. Eritrea – malaria prevalence survey 2002. Sintasath et al, 2005: 176 villages, 2,779 HH, 12,937 people. Overall prevalence 2.2%.

E N D
Effectiveness of malaria control in Eritrea, 1996 to 2003 Patricia M Graves June 6, 2008 IRI
Eritrea – malaria prevalence survey 2002 Sintasath et al, 2005: 176 villages, 2,779 HH, 12,937 people. Overall prevalence 2.2%
1a: Eritrea – malaria situationReported clinical malaria cases by age-group, Eritrea 1996 to 2003
Routine surveillance data • Can assist in: • Monitoring trends • Clarifying and measuring seasonality • Prioritizing areas for intervention • Defining and quantifying epidemics • Evaluating control measures
Source of cases dataset • 325 health facilities (1 to 9 per subzone) • Excluded: • National referral hospitals • Specialty clinics (ophthalmic and MCH) • Non-functioning facilities (no reports) • Private doctors • Worksite clinics • Remaining: 243 health facilities representing all subzones.
Focus on reported outpatient clinical malaria cases • Few facilities had diagnostics at start of period • Diagnostic capacity increased during study • Too few deaths and inpatients • Seasonal patterns clearly seen in clinical malaria cases • Inconsistency in lab forms for Pf/Pv.
Reported clinical malaria cases Incidence / 1000 / yr, 1998
Reported clinical malaria cases Incidence / 1000 / yr, 2000
Reported clinical malaria cases Incidence / 1000 / yr, 2002
Data sources used to analyze effectiveness of interventions • Datasets for 96 months (1998 to 2003), 58 subzones (districts) • Outpatient clinical malaria cases by month from new NHMIS (restricted here from 325 to 242 health facilities). • Satellite-derived rainfall (CPC CMAP 0407) and NDVI (version e from USGS/ADDS), averaged over subzone. • Amounts of interventions applied (IRS, ITNs, larval control)
Intervention data collected by subzone and month • Residual spraying (amount of chemical, people covered) • Number of impregnated nets issued and reimpregnated • Number of larval habitats eliminated • Chemical larviciding (number of sites, amount of chemical) • Treatments given by village health agents
Analysis • Outcome variable: number of clinical cases by subzone and month. • Cross-sectional multivariate time-series regression/ Poisson regression • First tested for ‘endogeneity’ (i.e. control being done in response to climate or increased case numbers) – no consistent pattern. • Independent variables expressed as ‘anomalies’ (deviations from subzone/calendar month means) to adjust for seasonality • Subzone fixed effect variables • Depreciation/cumulation of insecticides and nets • Climate variables as aggregated lags (Rain 2-3 months; NDVI 0-1 month.
Positive relationships between climate variables and malariacases (Anseba and Gash Barka) * p<0.05 *** p<0.001
Negative relationships between intervention variables and malaria cases * p<0.05 *** p<0.001
Eritrea analysis conclusions • Reduction in cases in Eritrea from 1998 to 2003 was not solely due to climate shifts. • Both IRS (with DDT or malathion) in one zone, and ITNs in two zones, were independently associated with reduction in cases. • There was evidence of effectiveness of larval control in one zone. • Better monitoring of interventions, especially larval control, is needed. • Routine malaria surveillance data (despite known drawbacks) is useful for evaluating the effectiveness of control measures, as long as climate variation is taken into account.