Download
1 / 1
60 likes | 1.08k Vues
Cetuximab in the treatment of rheumatoid arthritis: a case report Timothy Sullivan 1 ; John Deeken, MD 2 1 Georgetown University School of Medicine 2 Division of Hematology/Oncology, Georgetown University Hospital Georgetown University Background Discussion

E N D
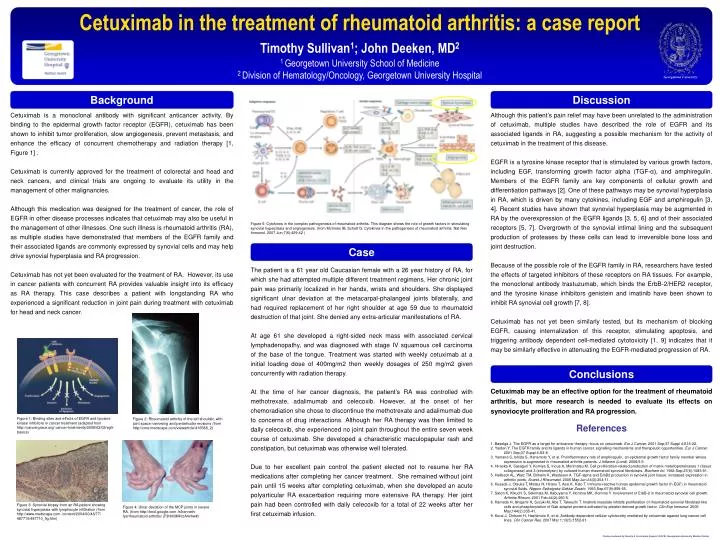
Cetuximab in the treatment of rheumatoid arthritis: a case report Timothy Sullivan1; John Deeken, MD2 1 Georgetown University School of Medicine 2 Division of Hematology/Oncology, Georgetown University Hospital Georgetown University Background Discussion Cetuximab is a monoclonal antibody with significant anticancer activity. By binding to the epidermal growth factor receptor (EGFR), cetuximab has been shown to inhibit tumor proliferation, slow angiogenesis, prevent metastasis, and enhance the efficacy of concurrent chemotherapy and radiation therapy [1, Figure 1] . Cetuximab is currently approved for the treatment of colorectal and head and neck cancers, and clinical trials are ongoing to evaluate its utility in the management of other malignancies. Although this medication was designed for the treatment of cancer, the role of EGFR in other disease processes indicates that cetuximab may also be useful in the management of other illnesses. One such illness is rheumatoid arthritis (RA), as multiple studies have demonstrated that members of the EGFR family and their associated ligands are commonly expressed by synovial cells and may help drive synovial hyperplasia and RA progression. Cetuximab has not yet been evaluated for the treatment of RA. However, its use in cancer patients with concurrent RA provides valuable insight into its efficacy as RA therapy. This case describes a patient with longstanding RA who experienced a significant reduction in joint pain during treatment with cetuximab for head and neck cancer. Although this patient’s pain relief may have been unrelated to the administration of cetuximab, multiple studies have described the role of EGFR and its associated ligands in RA, suggesting a possible mechanism for the activity of cetuximab in the treatment of this disease. EGFR is a tyrosine kinase receptor that is stimulated by various growth factors, including EGF, transforming growth factor alpha (TGF-α), and amphiregulin. Members of the EGFR family are key components of cellular growth and differentiation pathways [2]. One of these pathways may be synovial hyperplasia in RA, which is driven by many cytokines, including EGF and amphiregulin [3, 4]. Recent studies have shown that synovial hyperplasia may be augmented in RA by the overexpression of the EGFR ligands [3, 5, 6] and of their associated receptors [5, 7]. Overgrowth of the synovial intimal lining and the subsequent production of proteases by these cells can lead to irreversible bone loss and joint destruction. Because of the possible role of the EGFR family in RA, researchers have tested the effects of targeted inhibitors of these receptors on RA tissues. For example, the monoclonal antibody trastuzumab, which binds the ErbB-2/HER2 receptor, and the tyrosine kinase inhibitors genistein and imatinib have been shown to inhibit RA synovial cell growth [7, 8]. Cetuximab has not yet been similarly tested, but its mechanism of blocking EGFR, causing internalization of this receptor, stimulating apoptosis, and triggering antibody dependent cell-mediated cytotoxicity [1, 9] indicates that it may be similarly effective in attenuating the EGFR-mediated progression of RA. • Figure 5: Cytokines in the complex pathogenesis of rheumatoid arthritis. This diagram shows the role of growth factors in stimulating synovial hyperplasia and angiogenesis. (from McInnes IB, Schett G. Cytokines in the pathogenesis of rheumatoid arthritis. Nat Rev Immunol. 2007 Jun;7(6):429-42 ) Case The patient is a 61 year old Caucasian female with a 26 year history of RA, for which she had attempted multiple different treatment regimens. Her chronic joint pain was primarily localized in her hands, wrists and shoulders. She displayed significant ulnar deviation at the metacarpal-phalangeal joints bilaterally, and had required replacement of her right shoulder at age 59 due to rheumatoid destruction of that joint. She denied any extra-articular manifestations of RA. At age 61 she developed a right-sided neck mass with associated cervical lymphadenopathy, and was diagnosed with stage IV squamous cell carcinoma of the base of the tongue. Treatment was started with weekly cetuximab at a initial loading dose of 400mg/m2 then weekly dosages of 250 mg/m2 given concurrently with radiation therapy. At the time of her cancer diagnosis, the patient’s RA was controlled with methotrexate, adalimumab and celecoxib. However, at the onset of her chemoradiation she chose to discontinue the methotrexate and adalimumab due to concerns of drug interactions. Although her RA therapy was then limited to daily celecoxib, she experienced no joint pain throughout the entire seven week course of cetuximab. She developed a characteristic maculopapular rash and constipation, but cetuximab was otherwise well tolerated. Due to her excellent pain control the patient elected not to resume her RA medications after completing her cancer treatment. She remained without joint pain until 15 weeks after completing cetuximab, when she developed an acute polyarticular RA exacerbation requiring more extensive RA therapy. Her joint pain had been controlled with daily celecoxib for a total of 22 weeks after her first cetuximab infusion. Conclusions Cetuximab may be an effective option for the treatment of rheumatoid arthritis, but more research is needed to evaluate its effects on synoviocyte proliferation and RA progression. Figure 1: Binding sites and effects of EGFR and tyrosine kinase inhibitors in cancer treatment (adapted from http://cancergrace.org/ cancer-treatments/2009/03/02/egfr-basics) Figure 2: Rheumatoid arthritis of the left shoulder, with joint space narrowing and periarticular erosions (from http://cme.medscape.com/viewarticle/416588_2) References 1. Baselga J. The EGFR as a target for anticancer therapy--focus on cetuximab. Eur J Cancer. 2001 Sep;37 Suppl 4:S16-22. 2. Yarden Y. The EGFR family and its ligands in human cancer. signalling mechanisms and therapeutic opportunities. Eur J Cancer. 2001 Sep;37 Suppl 4:S3-8. 3. Yamane S, Ishida S, Hanamoto Y, et al. Proinflammatory role of amphiregulin, an epidermal growth factor family member whose expression is augmented in rheumatoid arthritis patients. J Inflamm (Lond). 2008;5:5. 4. Hiraoka K, Sasaguri Y, Komiya S, Inoue A, Morimatsu M. Cell proliferation-related production of matrix metalloproteinases 1 (tissue collagenase) and 3 (stromelysin) by cultured human rheumatoid synovial fibroblasts. Biochem Int. 1992 Sep;27(6):1083-91. 5. Hallbeck AL, Walz TM, Briheim K, Wasteson A. TGF-alpha and ErbB2 production in synovial joint tissue: increased expression in arthritic joints. Scand J Rheumatol. 2005 May-Jun;34(3):204-11. 6. Kusada J, Otsuka T, Matsui N, Hirano T, Asai K, Kato T. Immuno-reactive human epidermal growth factor (h-EGF) in rheumatoid synovial fluids. Nippon Seikeigeka Gakkai Zasshi. 1993 Sep;67(9):859-65. 7. Satoh K, Kikuchi S, Sekimata M, Kabuyama Y, Homma MK, Homma Y. Involvement of ErbB-2 in rheumatoid synovial cell growth. Arthritis Rheum. 2001 Feb;44(2):260-5. 8. Kameda H, Ishigami H, Suzuki M, Abe T, Takeuchi T. Imatinib mesylate inhibits proliferation of rheumatoid synovial fibroblast-like cells and phosphorylation of Gab adapter proteins activated by platelet-derived growth factor. Clin Exp Immunol. 2006 May;144(2):335-41. 9. Kurai J, Chikumi H, Hashimoto K, et al. Antibody-dependent cellular cytotoxicity mediated by cetuximab against lung cancer cell lines. Clin Cancer Res. 2007 Mar 1;13(5):1552-61. Figure 3: Synovial biopsy from an RA patient showing synovial hyperplasia with lymphocyte infiltration (from http://www.medscape.com /content/2004/00/48/77/ 487710/487710_fig.htm) Figure 4: Ulnar deviation of the MCP joints in severe RA. (from http://knol.google.com /k/kenneth-fye/rheumatoid-arthritis/ jF3hM3MH/zA4vhw#)