Download
1 / 27
360 likes | 2.08k Vues
Renal regulation of sodium balance. Stephen P. DiBartola, DVM Department of Veterinary Clinical Sciences College of Veterinary Medicine Ohio State University Columbus OH 43210. Renal handling of sodium. Sodium is filtered by the glomeruli and reabsorbed by the tubules

E N D
Renal regulation of sodium balance Stephen P. DiBartola, DVM Department of Veterinary Clinical Sciences College of Veterinary Medicine Ohio State University Columbus OH 43210
Renal handling of sodium • Sodium is filtered by the glomeruli and reabsorbed by the tubules • Energy for sodium transport in the kidney is required for the Na+-K+ ATPase located in the basolateral membranes of the tubular cells • Na+-K+ ATPase maintains the low intracellular sodium concentration that facilitates sodium entry at the luminal membranes
Renal handling of sodium • 67% of filtered load reabsorbed in proximal tubules • 25% of filtered load reabsorbed in loop of Henle • 5% of filtered load reabsorbed in distal convoluted tubule and connecting segment • 3% of filtered load reabsorbed in collecting duct
Mechanisms for sodium reabsorption differ in different parts of the nephron
Sodium reabsorption: Early proximal tubule • Luminal entry • Co-transport with glucose, amino acids, Pi • Na+-H+ antiporter • Basolateral exit • Na+-K+ ATPase • Tubular fluid Cl- concentration increases
Sodium reabsorption: Late proximal tubule • Luminal entry • Na+-H+ antiporter in parallel with Cl--Anion- antiporter (H+-Anion- recycled) • Basolateral exit • Na+ actively via Na+-K+ ATPase • Cl- passively via Cl- channel
Sodium reabsorption: Thin limb of Henle’s loop • Thin descending limb: Passive NaCl entry into tubular lumen • Thin ascending limb: Passive NaCl reabsorption
Sodium reabsorption: Thick ascending limb of Henle’s loop • Luminal entry • Na+-H+ antiporter • Na+-K+-2Cl- cotransporter (site of action of furosemide and bumetanide) • Basolateral exit • Na+-K+ ATPase • Tubular lumen strongly positive relative to peritubular interstitium
Sodium reabsorption: Distal convoluted tubule • Luminal entry • Na+-Cl- cotransporter (site of action of thiazide diuretics) • Basolateral exit • Na+ via Na+-K+ ATPase • Cl- via Cl- channel
Sodium reabsorption: Connecting segment and collecting duct • Luminal entry • Passively via Na+ channel (site of action of amiloride and triamterene) • Basolateral exit • Na+-K+ ATPase • Lumen-negative TEPD generated by Na+ movement facilitates Cl- reabsorption
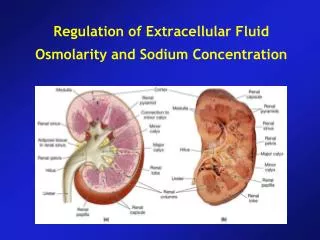
Renal regulation of sodium balance • Extracellular fluid volume is directly dependent on body sodium content • Adequacy of body sodium content is perceived as the fullness of the circulating blood volume (“effective circulating volume”)
Sensors for control of sodium balance • Low pressure mechanoreceptors (“volume” receptors) • Atria • Pulmonary vessels • High pressure baroreceptors (“pressure” receptors) • Aortic arch • Carotid sinus • Afferent arterioles of glomeruli
Effectors for control of sodium balance: the KIDNEY • Filtration? • NO: Autoregulation of GFR, tightly regulated serum Na+ concentration • Reabsorption? • YES: Several overlapping mechanisms insure control of Na+ balance
Control of renal sodium reabsorption • Glomerulotubular balance • Aldosterone • Peritubular capillary factors (Starling forces) • Other • Catecholamines • Angiotensin II • Atrial natriuretic peptide • “Pressure” natriuresis
Glomerulotubular balance • As spontaneous (primary) fluctuations in GFR occur, absolute tubular reabsorption of filtered solutes changes in a similar direction (i.e. the fraction of the filtered load that is reabsorbed remains constant) • This effect does NOT occur when a compensatory (secondary) fluctuation in GFR occurs in response to changes in sodium and water ingestion
Glomerulotubular balance: Mechanisms • Spontaneous increase in GFR would increase filtered load of glucose, amino acids, and phosphate, bicarbonate • Spontaneous increase in GFR would increase filtration fraction and alter peritubular Starling forces such that water and solute reabsorption in the proximal tubules would be facilitated
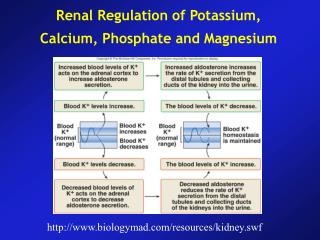
Aldosterone • Alters renal Na+ reabsorption in response to dietary fluctuations • Main stimuli for release: Angiotensin II, hyperkalemia, ACTH • Main effect: Increases number of open luminal Na+ channels and activity and number of basolateral Na+-K+ ATPase pumps in principal cells of collecting ducts
Think of the effects on P and Peritubular capillary factors (Starling forces) • Increased Na+ intake: ECF expansion • GFR & RPF increase proportionately (FF unchanged) • Decreased Na+ intake: ECF contraction • RPF decreases more than GFR (FF increased)
Peritubular capillary factors (Starling forces) Think of the effects on P & when FF increases • Increased Na+ intake: ECF expansion • GFR & RPF increase proportionately (FF unchanged) • Decreased Na+ intake: ECF contraction • RPF decreases more than GFR (FF increased)
Catecholamines • Efferent > afferent arteriolar constriction (increased FF) results in changes in peritubular Starling forces that facilitate Na+ reabsorption • Direct stimulation of proximal tubular Na+ reabsorption • Stimulation of renin release
Angiotensin II • Efferent > afferent arteriolar constriction (increased FF) results in changes in peritubular Starling forces that facilitate Na+ reabsorption • Direct stimulation of Na+-H+ antiporter in proximal tubules • Stimulates aldosterone secretion from adrenal glands
Atrial natriuretic peptide • Stimulus for release is atrial distension caused by volume expansion • Inhibits Na+ reabsorption in some parts of the collecting duct • Directly increases GFR • Inhibits renin and aldosterone secretion
“Pressure” natriuresis • Renal Na+ and water excretion are increased when renal arterial pressure increases without change in GFR • Mechanism is intra-renal and does not require neural or endocrine input
Regulation of water balance • Osmolality of ECF and serum sodium concentration are regulated by adjusting water balance • Water output: Anti-diuretic hormone (vasopressin) • Water intake: Thirst
Regulation of water balance • Sensors • Osmoreceptors in hypothalamus • Effectors • Anti-diuretic hormone (vasopressin) • Increases permeability of cortical and medullary collecting ducts to water and medullary collectiong ducts to urea
Stimuli for ADH release • Plasma hypertonicity (1 to 2% increase leads to maximal ADH release) • Volume depletion (5 to 10% decrease facilitates ADH release) • Other • Nausea • Pain • Anxiety • Drugs
Review of renin-angiotensin system (RAS) • Renin • Synthesized by granular cells of JGA • Release stimulated by decreased renal perfusion pressure, increased sympathetic tone, decreased delivery of Cl- to macula densa • Release inhibited by angiotensin II • Converts angiotensinogen to angiotensin I (A-I) • Angiotensin II • Prodcued by action of converting enzyme on A-I • Arteriolar vasoconstriction throughout body • Enhances renal excretion of Na+ and water