Download
1 / 44
460 likes | 867 Vues
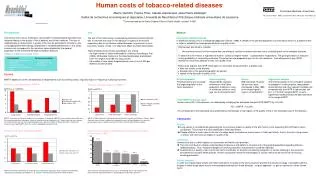
The Burden of Tobacco-Related Diseases and Health Care Costs of Tobacco Use in the Philippines. Marina Miguel-Baquilod, MD, MSc Country Research Coordinator, Tobacco and Poverty Study Department of Health, Manila . Background.

E N D
The Burden of Tobacco-Related Diseases and Health Care Costs of Tobacco Use in the Philippines Marina Miguel-Baquilod, MD, MSc Country Research Coordinator, Tobacco and Poverty Study Department of Health, Manila
Background Project: “Tobacco and Poverty Study” in the Philippines Component Studies: 1. Prevalence of Tobacco Use 2. Household Expenditures and Tobacco Use 3. Burden of Tobacco-Related Diseases in the Philippines 4. Analysis of Demand for Tobacco in the Philippines
Dept. of Health Dr. Marina M. Baquilod Dr. Ernie V. Vera Dr. Elizabeth R. Matibag WHO-TFI, HQ - Dr. Ayda A. Yurekli College of Public Health-University of Philippines, Manila Mr. Alvin G. Tan Prof. Marilyn E. Crisostomo . Dr. Jesus Sarol Dr. Jane C. Baltazar Collaborative Study Group
Demographic and Economic Profile, Republic of the Philippines • Population (2007)88.7M • Population of 15-64y.o.=59.2% of Total Popn. • Life Expectancy at birth, Projected 2007 (Male=66.11yrs; Female=71.64yrs) • Annual Growth Rate=2.4% • Poverty Incidence (2003)= 27.4% of Families • Unemployment (Jan.2007)7.8% • Ave. Family Income (2003)P147,888(U$2,640) • Ave. Family Expenditures (2003)P123,693 (U$2,208) • GNP (Q4’06)Php1,856.0B(U$37B) • GDP (Q4’06)Php1,693.6B(U$34B)
Health and Nutrition Status, 2003 • Infant Mortality Rate =30.0/1,000 Livebirths (Low/ High Income Ratio=2.16) • Chronic Undernutrition = 30% of children (0-5yrs old) • 6 of Top Leading Causes of Mortality were NCD’s (past 20yrs): Diseases of Heart and Vascular System, Cancers, COPD, Diabetes, and Kidney Diseases • Prevalence of Tobacco use, 34.8% (Male=56.5%; Female=12.1%), (Low/High Income Ratio=2.51)
Health Expenditures, Selected Western Pacfic Countries, 2002 Source: National Statistical Coordination Board, 2004
Rationale of the Study • In 1995, the World Bank, estimated the number of smokers to be 1.1 billion smokers worldwide and projected it to rise to 1.6 billion by 2025 (Jha and Chaloupka, 1999). • In low- and middle-income countries where, an estimated 930 million smokers belong, cigarette consumption has been noted to increase (Jha et al, 2002).
Rationale • Known to be associated with a number of medical and non-medical causes of death and disability (US DHHS, 2004; English et al, 1995; Doll et al, 2004), half of all smokers will eventually die prematurely because of their habit. • Half of these deaths occur in the middle age (39-65 years) and lose 20 to 25 years of productive life (Jha and Chaloupka, 1999). • It was estimated that in the year 2000, about 4.83 M premature deaths in the world would be attributable to smoking (Ezzati and Lopez, 2003).
Rationale • A significant number adult Filipinos (15yrs and above) currently smoke cigarettes or use any tobacco product (NNHeS1998, 2003; BRFS 2001); Prevalence of current tobacco use ranks next to China and Indonesia (Tobacco Atlas, 2003) • A considerable number of Filipino youth initiated to tobacco use; current smoking among girls had increased significantly (GYTS 2000, 2003).
Objectives • General objective: To determine the burden of disease attributable to smoking. • Specific objectives: • Determine the health impact attributable to tobacco-related diseases; • Determine the economic impact attributable to tobacco-related diseases.
Estimation of Disease Burden (Method 1) Population Attributable Risk where AB= attributable burden for a given risk factor and population AFj= fraction of the burden from cause j Bj = estimated population-level burden from cause j P = prevalence of the exposure RRj= relative risk of disease or injury from cause j in the exposed group compared to the unexposed group
Estimation of Disease Burden (Method 1) Smoking Impact Ratio CLC= Age-sex specific lung cancer mortality rate in a population NLC= Age-sex specific lung cancer mortality rate of never-smokers in the same population S*LC and N*LC = Age-sex specific lung cancer mortality rates for smokers and never-smokers in a reference population
Estimation of Disease Burden (Method 1) To correct for potential confounding, Murray and Lopez used this modified formula for the Relative Risk:
Estimation of Disease Burden (Method 2) SAF = [(p0 + p1(RR1) + p2(RR2)) - 1] / [p0 + p1(RR1) + p2(RR2)] P0=Percentage of adult never smokers in study group P1=Percentage of adult current smokers in study group P2=Percentage of adult former smokers in study group RR1=Relative risk of death for adult current smokers relative to adult never smokers RR2=Relative risk of death for adult former smokers relative to adult never smokers
Global Burden of Disease Study (1992): WHO & World Bank • To provide an objective assessment of health status that is comparable across countries • Address limitations of available health statistics • Disability Adjusted Life Years (DALY) as indicator
DALY • Measure of burden of disease as the gap between current health status and an ideal situation where people live to old age free of disease and disability. • Used for: 1. Measuring the health impact of a disease 2. Analyzing cost-effectiveness of alternative interventions 3. Priority setting • Combines life lost due to premature death with life years lost due to living in a disabled state.
DALY = YLL + YLD Where: YLL = Years of Life Lost or amount of time in years lost due to premature death from a specific disease. YLD = Years Lived with Disability or the period of time someone has to live suffering from a disability brought about by a specific disease.
Parameters for DALY Estimation- • Use of the spreadsheet model of Murray et. al. by triangulating data from various sources (sensitivity analysis): • Number of incident cases • Number of deaths • Number of cases with disabling sequelae • Duration of disability • Disability weights • Life expectancy • Age weighting • Discount rate
Estimation of Burden (DALY) Limited to four disease attributable to smoking namely: • Lung cancer • Chronic obstructive pulmonary disease (COPD) • Cerebro-vascular disease (CVD) • Coronary artery disease (CAD)
Estimation of Burden (Costs) • combination of review or records, literature review, and expert interviews. • Perspective-societal • Direct medical costs: hospitalization, out-patient consultations, diagnosis, treatment and rehabilitation costs • Direct non-medical costs (salaries of watchers, transportation costs, etc) were not included • Philippine Health Insurance Corporation (PHIC) provided another data source for hospitalization costs
Estimation of Burden (Costs) • Productivity losses due to premature deaths- years of life lost (YLL) with the daily* minimum wage (P325) projected to 20 years • Productivity losses due to the disease were estimated using work days lost due to the four diseases as reported by Dans and colleagues (unpublished).
Results *Data from NNHeS Dans et al, 2005
Results *Using SAMMEC methodology
Results **Using Peto-Lopez methodology
Results *Using SAMMEC methodology
Results **Using Peto-Lopez methodology
Results *Using SAMMEC Methodology
Results **Using Peto-Lopez Methodology
Results *Using SAMMEC Methodology figures
Results **Using Peto-Lopez Methodology figures
Discussion Limitations • Only four of the 40 known diseases to be caused by smoking were studied • Morbidity of the disease was probably underestimated using indirect estimation • Morbidity and mortality estimates did not include those for cigar smokers, passive smokers, pregnant women, and children • Minimum wage was used to estimate productivity losses • General picture of disease burden
Discussion • Higher estimates compared to Dans • steady increase of mortality rates from the four diseases studied • increasing population • YLL=437,710 (53.49/10,000) • Dans PYLL=125,918 (16.85/10,00) • 3.17 times Dans estimate
Discussion • DALYs from lung cancer and COPD mainly YLL • high case fatality ratio for lung cancer • CVD and CAD DALYs mainly YLD. • The long duration of CAD and CVD sequelae and their relatively low case fatality ratios
Discussion • Cost estimates • Low=$2.86 B (Php148.72 B) • High=$6.05 B (Php314.6 B) • Dans Estimate= $891 M (Php46 B) • GNP = Php 1,441.6B (2005 Q3) • GDP= Php 1,322.4B (2005 Q3) • Total Health Expenditure = Php165.2 B
Conclusions • DALYs range from 652,261 to 1,444,078 • Different composition of DALYs • Cost estimates range from $2.86 B to $6.05 B • Over half of cases of the 4 major diseases were attributable to smoking, hence, the significance of sustaining or strengthening comprehensive national tobacco prevention and control programs.
Policy Recommendations • Enforcement of the significant provisions of the Tobacco Regulatory Act of 2003 (RA 9211) and Framework Convention on Tobacco Control (FCTC) • Appropriation of budget, “Dedicated Taxes” as provided for in the “Sin Tax Law” (RA 9334), annual earmarking of 2.5% of revenues from tobacco excise tax since 2005 for disease prevention and control, focus on tobacco control and healthy lifestyle programs; and another 2.5% for Philippine Health Insurance, to increase coverage especially of indigent or poor families. • Strengthened comprehensive tobacco control programs that should prevent youth and poor people from uptake (taxation), available and accessible smoking- cessation programs, and strict environmental policies and regulations to prevent second-hand exposure to tobacco smoke.
Tobacco Free Initiative, WHO, HQ - Dr. Anne- Marie Perucic - Dir. Douglas Bettcher WHO,WPRO Mr. Burke Fishburn Mr. Jonathan Santos WR-Philippines -Dr. Jean-Marc Olive -Dr. John Juliard Go DOH - Usec. Ethelyn Nieto - Director Eric Tayag - Director Yoly Oliveros - Director Maylene Beltran - Dr. Marvi Ala - Dr. Jessica de Leon Other GO’s - NSO, NSCB, NEDA, NTA, BIR Acknowledgments
MARAMING SALAMAT! Support Tobacco-Free Philippines