Download
1 / 30
300 likes | 594 Vues
SR Simon, JH Gurwitz, KA Chan, SB Soumerai, AK Wagner, SE Andrade, AC Feldstein, ... Raebel, MA, Lyons EE, Simon SR, et al. Lab Monitoring of High Risk ...

E N D
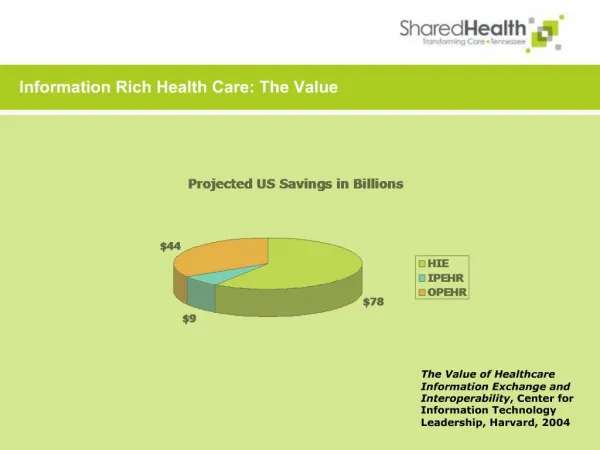
Slide 1:The Value of Health Information Technology in Improving Pharmacotherapy
Steven R. Simon, MD, MPH Harvard Medical School and Harvard Pilgrim Health Care
Slide 2:Objectives
Problems with drug therapy in the elderly Overuse Underuse Misuse HIT-based interventions Expanding HIT: Role of QIOs Non-HIT based interventions
Slide 3:Potentially Inappropriate Medication Use Among Elderly Persons in US HMOs, 2000-2001
SR Simon, JH Gurwitz, KA Chan, SB Soumerai, AK Wagner, SE Andrade, AC Feldstein, JE Lafata, R Platt
Slide 4:Sample Description
Sample Age 65+ Eligible* *Eligibility Criteria: Age 65 years or older on January 1, 2000; continuously enrolled 1/1/00 � 6/30/01; continuous drug benefit during study period Total Eligible: 157,517
Slide 6:Overall, 28.8% received 1 or more potentially inappropriate agent
Slide 7:Underuse of Medications in the Elderly
asthma cardiovascular disease depression dyslipidemia hypertension osteoporosis prevention pain management stroke prevention
Slide 8:Underuse of Statins
Evidence-based guidelines (NCEP): aggressive statin use to lower cholesterol Slow adoption of statins in early 1990s Among patients with AMI in 37 Minnesota hospitals in 1995, 37% received LLDs (Majumdar et al, JGIM 1999) Among elderly Medicare patients with CHD in 1997: 4.1% of patients with Medicare only on statins 27.4% of patients with employee-sponsored insurance on statins. (Federman et al, JAMA 2001)
Statin Use among Patients with CHD or MISlide 11:Examples of Misuse
Drug-drug interactions Drug-allergy interactions Drug-disease interactions (e.g., renal dosing) Inadequate laboratory monitoring Prescribing, transcribing, dispensing errors Wrong drug Wrong dose Wrong route
Slide 12:Lab Monitoring of High Risk Drugs at Initiation of Therapy
Objective: Describe baseline lab monitoring among new users of HRDLMs N=2,000,000 (200,000 x 10 HMOs) 36 drugs/classes requiring monitoring ACE-inhibitors (Creatinine, K+) Amiodarone (liver, thyroid function) Lab monitoring error: No test 180 d before or 14 d after initiation. Raebel, MA, Lyons EE, Simon SR, et al.
Slide 13:Lab Monitoring of High Risk Drugs at Initiation of Therapy
Overall error rate: 38.6% 107,791 / 279,418 dispensings 39.2% starting ACEi did not have creatinine and K+ 57.2% starting amiodarone did not have liver and thyroid function tests Raebel, MA, Lyons EE, Simon SR, et al.
Slide 14:Interventions: HIT-based
Bates, D. W. et al. N Engl J Med 2003;348:2526-2534 Warning Displayed for a Drug Allergy BMJ. 2002;325:491�7.Slide 20:Expanding HIT: Role of QIOs
Slide 21:Increasing EHR Adoption in Massachusetts
Goal: To improve the safety of patient care delivered by every outpatient provider in Massachusetts Approach: Develop partnership among key stakeholders Implementation: Staged over 5 years
Slide 22:Components of Initial Proposal
Build consensus among key stakeholders Identify vendors of computer hardware and EMR software interested in collaborating with Massachusetts Low number, ideally 2-4
Slide 23:Components of Initial Proposal
Identify purchasers or business groups willing to pay a premium to providers who are willing to make or have already made the transition to electronic records Identify incentive package that will make it attractive for providers to adopt
Slide 24:Role of QIOs
Establish consensus on quality measures Collect automated (EHR) quality data from practices Channel data to incentive-paying mechanism Use data to implement QI programs Broadly At level of individual practice (or provider?) Role in recruitment, implementation, evaluation, other?
Slide 25:Non-HIT-based Interventions to Change Prescribing Behavior
Mailed information Audit and Feedback Opinion Leaders Academic Detailing
Slide 26:A Cluster-Randomized Controlled Trial of Individual versus Group Academic Detailing to Improve the Use of Antihypertensive Medications in Primary Care
Supported by a cooperative agreement from the Agency for Healthcare Research and Quality SR Simon, SR Majumdar, KP Kleinman, S Salem-Schatz; C Warner; L Prosser; I Miroshnik, SB Soumerai
HCHP (1995) 47 practice groups 9 practice groups randomized Individual Academic Detailing (N=3) Group Academic Detailing (N=3) Mailed Practice Guidelines (N=3) 114 Clinicians and 1066 HTN patients 120 Clinicians and 1007 HTN patients 133 Clinicians and 1619 HTN patientsSlide 28:Academic Detailing Interventions
Single educational outreach visit Trained physician-educator (detailer) Objective Address and overcome barriers to prescribing diuretics and beta blockers Credible messenger Unbiased information Individual or small group (N=6-8) visits
Slide 29:Absolute increases in unadjusted rates of use of diuretics or �-blockers among patients with incident hypertension
Year 1 Year 2 Baseline Rates (58%) (59%) (58%) (58%) (59%) (58%)
Slide 30:Take-Home Messages: Improving Drug Therapy in the Elderly
Serious and widespread problems Overuse, underuse, misuse HIT-based interventions promising Need for expansion of HIT, especially EHRs Continued need for non-HIT-based interventions E.g., academic detailing