Download
1 / 53
530 likes | 822 Vues
Alcoholic Liver Disease. July/August 2013 issue of Radiologic Technology. Directed Readings In the Classroom. Instructions:.

E N D
Alcoholic Liver Disease July/August 2013 issue of Radiologic Technology Directed Readings In the Classroom
Instructions: • This presentation provides a framework for educators and students to use Directed Reading content published in Radiologic Technology. This information should be modified to: • Meet the educational level of the audience. • Highlight the points in an instructor’s discussion or presentation. • The images are provided to enhance the learning experience and should not be reproduced for other purposes.
Introduction • In the United States, approximately 100 000 deaths are attributed to alcohol abuse each year. In 2009, the World Health Organization listed alcohol use as one of the leading causes of the global burden of disease and injury. Alcoholic liver disease, a direct result of chronic alcohol abuse, insidiously destroys the normal functions of the liver. The end result of the disease, cirrhosis, culminates in a dysfunctional and diffusely scarred liver. • This article discusses the clinical manifestations, imaging considerations, and treatment of alcoholic liver disease and cirrhosis. Normal liver function, liver hemodynamics, the disease of alcoholism, and the deleterious effects of alcohol also are reviewed.
Embryonic Development • The liver initially develops from the foregut, an element of the early primitive gut, within the first few weeks of embryonic development. In the embryo, the liver is responsible for hemopoiesis, which is the formation and development of blood cells. The primary liver cells, the hepatocytes, form a series of branching and anastomosing plates that constitute the normal hepatic architecture.
Embryonic Development • The tiny umbilical vein of the umbilical cord provides perfusion to the developing liver. The umbilical vein enters the fetus superior to the bladder and travels cephalically toward the liver. At the liver, the umbilical vein bifurcates into right and left branches. The left branch enters the liver and attaches directly to the left portal vein. The right branch is essentially a shunt between the umbilical vein and the inferior vena cava. This shunt, referred to as the ductusvenosus, allows some blood to bypass the liver and flow directly into the fetal inferior vena cava (IVC). Once in the IVC, the blood can travel up to the fetal heart and be dispersed throughout the fetus.
Embryonic Development • Shortly after birth, the ductusvenosus collapses and becomes the ligamentumvenosum. Concurrently, the right branch of the umbilical vein collapses. The remaining structure of the umbilical vein then is referred to as the round ligament or the ligamentumteres. The umbilical vein can recanalize, or reopen, and shunt blood away from a liver that has been damaged. This condition, known as portal hypertension, will be reviewed further in this article when common complications of alcoholic liver disease (ALD) and cirrhosis are discussed.
Anatomy and Physiology of the Liver • The liver is the largest parenchymal organ of the body. Located within the right upper quadrant and extending across the midline of the body, the normal liver occupies 2 distinct abdominal regions — the right hypochondrium and epigastrium. Anatomically, the liver consists of 3 primary lobes, which can be differentiated by surrounding landmarks and location. The largest, the right lobe, occupies much of the right upper quadrant. The left lobe of the liver is located within the midline of the abdomen. This lobe can traverse the midline and may come in contact with the spleen. The third, and much smaller lobe, is the caudate lobe. The caudate lobe is located posterior to the left lobe, and is therefore located within the midline of the abdomen as well.
Anatomy and Physiology of the Liver • The liver performs many vital functions that sustain life, including: • Digestion. • Excretion. • Nutrient storage and conversion. • Detoxification of destructive chemicals. • The creation of new molecules.
Anatomy and Physiology of the Liver • The liver consists of several types of specialized cells that sustain homeostasis, the body’s ability to preserve internal stability. Externally, the liver has a protective covering referred to as the Glisson capsule. Within the capsule, nearly 100 000 groups of cells referred to as lobules create the mass of the liver.The primary cells contained within these liver lobules are referred to as hepatocytes. Hepatocytes are responsible for adjusting secretion and absorption levels of nutrients within the liver and comprise 70% to 80% of the liver mass. Hepatocytes are unique in that they have long life spans and cannot only respond to disease, but in many cases restore previously damaged hepatic tissue.
Anatomy and Physiology of the Liver • The nonparenchymal cells of the liver include Kupffer cells, endothelial cells, hepatic stellate cells, and pit cells. The Kupffer cells perform significant phagocytic functions, such as demolition of pathogens, removing cell debris, and destruction of dysfunctional or damaged red blood cells. The crucial role that Kupffer cells play in the hepatic reaction to alcohol and its metabolites will be discussed further in this article.
Hemodynamics of the Liver • Appreciating the normal blood flow within the liver is important because hepatic perfusion is compromised with many forms of liver disease. The hemodynamics of the liver are distinctive chiefly because unlike many organs, the liver has a dual blood supply. The liver receives most of its blood flow, approximately 70%, from the main portal vein, which enters at the hilum of liver, an area also referred to as the portahepatis. • The main portal vein bifurcates within the liver into right and left portal vein branches. The portal veins have minimal pulsatility when examined with ultrasonography and pulsed-wave Doppler.
Hemodynamics of the Liver • A supplementary blood supply to the liver, the hepatic artery, originates from the anterior aspect of the abdominal aorta via a branch called the celiac artery (also called the celiac trunk or celiac axis). The hepatic artery is one of 3 branches of the celiac artery. The hepatic artery bifurcates once inside the liver into right and left branches. • Filtered blood exits the liver by means of the hepatic veins. There are typically 3 hepatic veins: middle, right, and left. These veins often are used to differentiate the 2 main lobes of the liver and further separate these lobes into segments. The hepatic veins empty the filtered blood from the liver into the IVC.
Assessing Normal Liver Function • Serum liver function tests are a common clinical assessment used by physicians to assess general well-being. A liver function blood test includes a laboratory assessment of several levels, including an evaluation of: • Alanine aminotransferase. • Aspartate aminotransferase. • Alkaline phosphatase. • Bilirubin. • Albumin. • Total protein.
Assessing Normal Liver Function • Of some importance to imaging professionals is the physical manifestation of elevated bilirubin. Bilirubin, a major component of bile, is the byproduct of hemoglobin breakdown. An elevation in bilirubin can result in jaundice, which is the yellowing of the skin and sclera of the eyes. Consequently, imaging professionals should be capable of recognizing jaundice in patients that present with elevated liver function test.
Hepatic Imaging Features • Ultrasonography provides a noninvasive, nonionizing, effective means of evaluating the liver. The normal echotexture of the liver is said to be smooth and homogeneous, consisting of medium-to-low echoes, only occasionally disrupted by the hepatic vasculature and normal hepatic fissures and ligaments. Representative images demonstrate the hepatic and portal veins, the interface between the liver and right kidney, and the hepatic lobes. An assessment of the biliary tract, including the gallbladder, often is performed as well.
Hepatic Imaging Features • Computed tomography (CT) frequently is used to assess hepatic maladies. Unenhanced CT readily demonstrates the homogeneous parenchyma of the normal liver. The appearance of the attenuation value of the unenhanced liver is often greater than the spleen; although with contrast, this varies according to the time of image acquisition. However, immediately after contrast administration, the attenuation value of the liver often becomes less than that of the spleen.
Alcoholism and the Effects of Alcohol • In 2009, the World Health Organization listed alcohol use as one of the leading causes of the global burden of disease and injury, surpassed only slightly by childhood malnourishment and unsafe sex. This placed alcohol use ahead of unsafe water and sanitation, hypertension, high cholesterol, and tobacco use, and clearly affirms that alcohol is the most widely abused substance in the world. • In the United States, approximately 100 000 deaths per year are attributed to alcohol abuse. Alcohol use is an underlying cause of more than 30 conditions and a definite contributing factor to many more, including psychotic disorder, alcoholic cardiomyopathy, amnesic syndrome, and alcoholic liver disease. Alcohol consumption is the leading cause of liver disease in the United States, with approximately 40% of deaths from cirrhosis attributed to alcohol-induced liver disease.
Alcoholism and the Effects of Alcohol • The Mayo Clinic defined alcoholism as a chronic disease in which the body becomes reliant upon alcohol (ethanol). Furthermore, it has been referred to as a syndrome that consists of 2 phases: problem drinking and alcohol addiction. • Problem drinking: characterized by consumption that is used to deal with stressors and anxiety. • Alcohol addiction: described by the American Psychiatric Association as a disease in which individuals become preoccupied with drinking, have impaired control over drinking, suffer from compulsive drinking, drink despite physical or psychological problems caused by drinking, and have a tolerance for alcohol, and/or suffer from withdrawal symptoms.
Alcoholism and the Effects of Alcohol • In the United States, 67% of the population aged 18 years or older drink alcohol, while nearly 18 million Americans suffer from alcoholism or alcohol-related health issues. A 2008 study performed by the National Survey on Drug Use and Health claimed the rate of youth alcohol consumption among those aged 12 to 17 years was 14.6%. In addition, 70% of 8th graders, 84% of 10th graders, and 88% of 12th graders have at least tried an alcoholic beverage. It is important to note that 22 is the average age when alcohol dependency begins.
Alcoholism and the Effects of Alcohol • A standard alcoholic beverage has been described as any drink that contains 14 g of pure alcohol. Therefore, the list includes a single 12 floz can of beer, 5 floz of table wine, or a 1.5 floz shot of 80-proof spirits. • Irrespective of what form of alcohol is consumed, the greatest risk factor appears to be the quantity of alcohol consumed. The definition for low-risk drinking for men and women differs, because women suffer from hepatic damage and cirrhosis with considerably smaller amounts of alcohol consumption. Thus, a man should not drink more than 4 drinks per day and no more than 14 drinks per week. A woman should not drink more than 3 drinks per day and no more than 7 drinks per week. • However, we still have limited knowledge of the pathological factors that cause liver damage, and there appears to be no “safe” limit for alcohol consumption.
Alcohol Metabolism and the Liver • The liver is the principal organ for alcohol metabolism. The body naturally recognizes ethanol alcohol as a foreign, toxic agent that can disrupt normal homeostasis. • When we consume ethanol, it is rapidly absorbed by the upper gastrointestinal tract. Ethanol is diffused throughout the body, but exposure is greatest to the liver, via the main portal vein. Ethanol is metabolized by the body in the gastric mucosa and the liver. These organs manage an enzyme referred to as alcohol dehydrogenase, which is used by the body to oxidize ethanol and convert it into acetaldehyde and other metabolites. Acetaldehyde ultimately is converted by the body into acetic acid, and then acetate. Acetaldehyde affects protein synthesis.
Alcohol Metabolism and the Liver • Alcohol’s metabolites, especially acetaldehyde, damage vital liver cells because of the excessive generation of free radicals (molecules with unpaired electrons). One destructive byproduct is the reactive oxygen species of free radicals. An excessive amount of this type of toxic free radical causes oxidative stress, which results in the body’s inability to prevent and repair hepatic damage and the destruction of deoxyribonucleic acid.
Alcohol Metabolism and the Liver • Alcohol metabolism differs dramatically between sexes. Women are much more likely to suffer from liver damage than men as a result of alcohol consumption. However, this phenomenon is not clearly understood. • Nonetheless, an estimated 5.3 million women in the United States drink in a manner that is harmful to their health. In addition to sex, the incidence of liver damage depends on the individual’s ethnicity, genetic predisposition, and nutritional state.
Alcohol Metabolism and the Liver • In addition to the immediate damage of acetaldehyde and the free radicals, the phagocytic cells of the liver, the Kupffer cells, also mount an immune response. This response is the result of an increase in toxins in the blood that leak from the intestinal wall and enter the bloodstream because of alcohol consumption.The activation of Kupffer cells is responsible for early ethanol-induced liver injury. In fact, through an intricate chain of events, it is the activation of Kupffer cells that ultimately leads to the death of hepatocytes.This damage results in the manifestation of alcoholic liver disease, and eventually to the development of fibrosis, or scar tissue, within the liver.
Alcoholic Liver Disease and Alcoholic Cirrhosis • ALD is caused by alcoholism and can be divided into 3 types: hepatic steatosis, alcoholic hepatitis (inflammation), and cirrhosis. It is important to note that the components of ALD can be seen independent of alcohol consumption and it appears that they are not part of a continuum. • The mechanism behind the development of ALD is not completely understood, because it is estimated that only 10% to 20% of alcoholics develop cirrhosis. However, it is suspected that if other risk factors are present, such as obesity and hepatitis C, there may be increased likelihood of progression to cirrhosis.
Alcoholic Liver Disease and Alcoholic Cirrhosis • Hepatic steatosis, commonly referred to as fatty liver, is a frequent diagnosis that is not exclusive to patients suffering from ALD. Fatty liver is the accumulation of triglycerides in the hepatocytes. Fatty liver has been demonstrated in 90% to 100% of all heavy drinkers. Short-term exposure to 80 g of alcohol (about 8 beers) over several days can produce hepatic changes consistent with fatty liver disease. • Fatty liver disease can be reversed if alcohol consumption is stopped or significantly reduced. However, there are often no clinical symptoms, so fatty liver may be undiagnosed. Although fatty liver may lead to an elevation in laboratory findings, it is often diagnosed with imaging when the patient presents with unrelated symptoms.
Alcoholic Liver Disease and Alcoholic Cirrhosis • Hepatitis is inflammation of the liver. In the Western world, fatty liver with the development of hepatitis, referred to as steatohepatitis, has been acknowledged as a precursor for the development of cirrhosis. • Alcoholic hepatitis results directly from alcohol abuse and is observed in as many as 35% of heavy drinkers. Like other forms of hepatitis, alcoholic hepatitis can be subclinical. Laboratory findings are more predictive if the disease has progressed. • Approximately 40% of patients with alcoholic hepatitis who continue to drink will develop alcoholic cirrhosis within 1 to 2 years.
Alcoholic Liver Disease and Alcoholic Cirrhosis • Hepatocellular death with resulting fibrosis and regeneration is collectively referred to as cirrhosis. Cirrhosis slowly destroys normal hepatic architecture by interspersing fibrous bands of connective tissue between the hepatic lobules, which results in the regeneration of liver cells in nodules that are unrelated to normal vasculature. • A specific causative form of cirrhosis, alcoholic cirrhosis, is defined as a condition in which there is continuing fibrosis resulting in the subdivision of the liver into nodules of proliferating hepatocytes surrounded by scar tissue as the direct result of chronic alcohol abuse.Alcoholic cirrhosis is a debilitating disease that remains among the top 10 causes of death worldwide, and the 12th leading cause of death in the United States.
Alcoholic Liver Disease and Alcoholic Cirrhosis • Alcoholic cirrhosis is an irreversible condition that has an estimated frequency of 10% to 15% among people who consume 50 g of alcohol daily over a 10-year period. It is characterized by both steatosis and hepatitis, and fibrosis. If left unchecked and untreated, inflammation of the liver certainly produces hepatic fibrosis.
Alcoholic Liver Disease and Alcoholic Cirrhosis • The principal pathogenetic process in the development of cirrhosis is the progressive fibrotic changes that occur within the liver parenchyma combined with the disruption of the normal hepatic vasculature. The fibrous tissue found in the liver with cirrhosis is formed from the abnormal accumulation of a naturally occurring substance, collagen. Excessive collagen is produced by the liver’s hepatic stellate cells as a result of complex cellular changes from acetaldehyde exposure. This accumulation of fibrotic tissue impedes normal liver function and distorts normal hepatic architecture, thus leading to the manifestation of cirrhosis. The liver becomes smaller, harder, and difficult to perfuse with blood. The other characteristic of cirrhosis in addition to fibrosis is the manifestation of regenerating nodules. The histologic classifications of cirrhosis include micronodular (chronic), macronodular (acute), and mixed forms of cirrhosis.
Alcoholic Liver Disease and Alcoholic Cirrhosis • The early stages of cirrhosis are referred to as compensated cirrhosis. In these stages, the liver, though permanently scarred, can perform many of its vital functions. The final stages of cirrhosis are referred to as decompensated cirrhosis. With decompensated cirrhosis, the liver is irreparably scarred and hepatic function is compromised. • While patients with compensated cirrhosis can have the same survival as the general population, those with decompensated cirrhosis have a median survival of less than 2 years. It is important to note that patients with alcoholic hepatitis can present with clinical features similar to decompensated cirrhosis.
Alcoholic Liver Disease and Alcoholic Cirrhosis • There are 4 stages of cirrhosis according to criteria agreed upon by the Baveno IV conference: • Stage 1: uncomplicated cirrhosis. • Stage 2: cirrhosis with evidence of esophageal varices but without bleeding and ascites. • Stage 3: cirrhosis with ascites, with or without esophageal varices. • Stage 4: cirrhosis with gastrointestinal bleeding, with or without ascites. • Stages 1 and 2 correspond with compensated cirrhosis, while stages 3 and 4 correspond with decompensated cirrhosis. Hepatic failure occurs when 80% to 90% of hepatic function is lost.
Sequelae and Complications of Alcoholic Cirrhosis • The most common result of alcohol cirrhosis is a hemodynamic shift referred to as portal hypertension. Portal hypertension is the elevation of the blood pressure within the portal venous system. It develops as a result of the resistance to normal blood flow to the liver via the main portal vein. In turn, this resistance leads to elevated pressure within the portal veins and an enlargement of the main portal vein. The development of portal hypertension is the earliest and most important complication of cirrhosis because most of the physical problems associated with cirrhosis are attributable to it.
Sequelae and Complications of Alcoholic Cirrhosis • As the resistance within the portal vein increases, small tributaries between the portal and systemic circulation develop. These are referred to as portosystemic venous collaterals or portosystemic shunts. One location for portosystemic shunts is the paraumbilical vein, which collapses shortly after birth and becomes the ligamentumteres. In patients with portal hypertension, the paraumbilical vein may recanalize, or reopen, and blood is once again shunted away from the liver. This is referred to as portosystemic shunting.
Sequelae and Complications of Alcoholic Cirrhosis • Although these tiny tributaries are vital for the patient suffering from portal hypertension, they are highly prone to rupture. • Gastroesophagealvarices are found in 65% of patients with advanced cirrhosis. These fragile vessels rupture and lead to acute hemorrhage and death in about half of patients. In some cases, hepatofugal flow occurs within the portal veins. Hepatofugalflow is a reversal of flow; therefore, instead of forward flow toward the liver, the portal veins flow away from the liver.
Sequelae and Complications of Alcoholic Cirrhosis • Portal hypertension is a frequent cause of ascites in patients with cirrhosis. Ascites is defined as the pathological accumulation of fluid within the peritoneal cavity. Ascites develops as a result of the buildup of fibrous tissue within the liver, increasing hydrostatic pressure and the leakage of serous fluid from the cells. Occasionally this fluid becomes infected, resulting in a condition known as spontaneous bacterial peritonitis. This infection may be the result of bacteria translocating from the intestines to the ascites via the lymphatic channels or bloodstream. Concurrently, enlargement of the spleen, referred to as splenomegaly, is a common finding in patients with portal hypertension and cirrhosis.
Sequelae and Complications of Alcoholic Cirrhosis • Patients often suffer from hepatic encephalopathy as well, which is a brain abnormality caused by the liver’s inability to remove toxins, specifically ammonia, from the blood. These patients can suffer from a wide range of central nervous system abnormalities that include day-night reversal, mild intellectual impairment, and even coma. • Hepatorenal syndrome is another complication of advancing cirrhosis. It is described as dysfunction of the kidneys characterized by reduced renal circulation, retention of sodium and water, and excess urea in the blood.
Sequelae and Complications of Alcoholic Cirrhosis • Cancer is a leading cause of death for patients with cirrhosis. There appears to be a definite connection between long-standing cirrhosis and the most common form of liver cancer, hepatocellular carcinoma (HCC). Patients who drink more than 80 g of alcohol per day for more than 10 years have a 5-fold increase in the risk for HCC. • Clinical findings of HCC include abdominal distention, abdominal discomfort, anorexia, and an elevated serum alpha-fetoprotein.
Clinical Features and Diagnosis of Cirrhosis • The clinical signs of cirrhosis can range from subtle onset to acute manifestations that may cause irreversible physical debilitation. The vague, nonspecific early signs and symptoms of cirrhosis include weakness, malaise, disrupted sleep, muscle cramps, and weight loss. As the disease progresses, the individual suffers from jaundice, ascites, and peripheral edema. These clinical features result from hepatic cell dysfunction, and most often are the result of portal hypertension and portosystemic shunting.
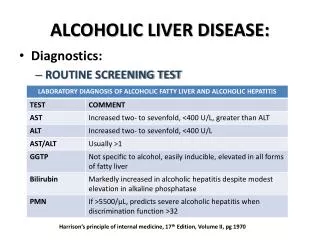
Clinical Features and Diagnosis of Cirrhosis Laboratory findings for cirrhosis are also nonspecific. However, there are common indicators that point to hepatic damage. Gamma glutamyltransferase (y-GT), also referred to as gamma-glutamyltranspeptidase, is a liver enzyme that is especially sensitive for ALD. The Child-Pugh-Turcotte scoring system for staging cirrhosis, which includes both laboratory and clinical findings, has a sensitivity and specificity of 78% and 83%, respectively. This scoring method evaluates the bilirubin, albumin, and prothrombin laboratory findings. It also includes an evaluation for ascites and encephalopathy.
Clinical Features and Diagnosis of Cirrhosis Alcoholic cirrhosis can be suspected clinically in the presence of risk factors such as obesity and chronic alcohol consumption. Diagnosis can be based on the presence of ascites, varices, and spider angiomas. However, liver biopsy remains the most definitive tool for confirming hepatic scarring and vascular compromise.
The Role of Imaging in Diagnosing Cirrhosis • Ultrasonography and CT play a vital function in the early detection of alcoholic cirrhosis, associated abnormalities, and further assessment of cirrhosis. The sonographic appearance of cirrhosis has been well documented. Features include: • Nodular hepatic architecture. • Atrophic right lobe. • Enlarged caudate lobe and left lobe. • Difficult-to-penetrate liver. • Increased echogenicity (in the presence of fatty infiltration). • Coarse, heterogeneous echotexture. • Ascites.
The Role of Imaging in Diagnosing Cirrhosis Patients with elevated liver functions should be closely examined with ultrasonography for signs of cirrhosis. Some institutions use ultrasonography for the initial identification of hepatic architectural changes. Hepatomegaly can be an early manifestation of the disease, as with other instances of hepatitis. Further investigation of the abdomen with ultrasonography may yield evidence of splenomegaly and ascites. It is important to note that sonographers must further examine the liver for signs of portal hypertension and HCC whenever signs of cirrhosis are identified.
The Role of Imaging in Diagnosing Cirrhosis Evidence of portosystemic shunting can be visualized with ultrasonography as well. The transjugular intrahepatic portosystemic shunt (TIPS) is an exceedingly effective treatment for patients suffering from unmanageable variceal bleeding and ascites. Ultrasonography is used following placement to document the stent’s patency.
The Role of Imaging in Diagnosing Cirrhosis • CT is also useful for evaluating liver disease. CT imaging features of cirrhosis include: • Nodular hepatic architecture. • Atrophic right lobe. • Enlarged caudate lobe and left lobe. • Evidence of confluent hepatic fibrosis. • Heterogeneous texture. • Ascites. • Splenomegaly. • Portosystemic collateral vessels.
The Role of Imaging in Diagnosing Cirrhosis Interventional radiologists may perform an assessment of the hepatic venous pressure gradient (HVPG). HVPG is the gold standard for assessing the severity of portal hypertension. This is an invasive procedure performed under fluoroscopic guidance in which a balloon-tipped catheter is advanced into the right hepatic vein via the internal jugular vein. At this point, the hepatic venous pressure is measured using an electromechanical transducer and polygraph. Although HVPG remains the best way to assess the degree of portal hypertension, ultrasonography has potential to provide a noninvasive and highly efficient alternative.
Treatment and Prognosis Abstinence from alcohol consumption is the most obvious treatment for ALD, although it is difficult for many patients. For patients with alcoholic cirrhosis who stop drinking, 90% live for another 5 years, while those who continue to drink have a 70% chance of living less than 5 years. In those who abstain from alcohol consumption, less severe fatty liver disease can be reversed in a few weeks, while resolution of alcoholic hepatitis can take more than 6 months. A TIPS, as mentioned earlier, is an effective means of treatment for unmanageable ascites. For severe liver damage and severe alcoholic hepatitis, corticosteroid treatment may be used to reduce the inflammatory response.
Treatment and Prognosis Liver transplant is a controversial treatment for patients with alcohol-induced liver disease. Some people hold negative views concerning alcoholics receiving liver transplants because they believe that alcoholics bear full responsibility for their illness. Nevertheless, liver transplants for ALD patients are often more successful than in patients requiring a liver transplant because of other diseases. Most ALD patients who undergo a liver transplant are younger than 60 years of age and are suffering severe liver impairment. Patients are advised to be abstinent for at least 6 months prior to surgery. Many complications of liver transplantation exist, including recurrence of hepatocellular carcinoma and graft rejection. However, 5-year survival rates have been reported to be as high as 80%.
Treatment and Prognosis There is current research on new approaches to treat or reverse hepatic fibrosis. Of interest is the inverse relationship between coffee intake and the risk of cirrhosis. Coffee intake has a favorable effect on alcohol-related cirrhosis risk. One study evaluated more than 700 individuals and determined that espresso coffee represented a definite modulator of alcoholic cirrhosis risk, although the connection is not clearly understood. The prognosis for patients with alcoholic cirrhosis depends on several factors. Cirrhosis mortality rates are often 2 times higher in men than women, although at any given level of alcohol consumption, women have a higher likelihood of developing cirrhosis than men.
Treatment for Alcoholism • It is important to keep in mind that alcoholism has a wide range of negative effects, not only on the individual, but on his or her family, friends, and even strangers. • The Center for Substance Abuse Prevention offers information on all aspects of alcohol abuse and other types of drugs. If you suspect that alcoholism is having a negative effect on you or a loved one, it is vital to remember that prevention, recognition, and early prevention, and treatment are key. A simple screening tool for alcoholism, the CAGE questionnaire, is often used by primary care physicians. It also can be used by individuals who suspect that they or a family member may be suffering from alcoholism.