Download
1 / 47
500 likes | 952 Vues
Health Inequities What they are… Why they are… Where they are… How to address them… Anthony Fleg, UNC volunteer Goals for the training Inspiration to work/volunteer to address issues of inequ it ies Greater understanding of inequities in health

E N D
Health Inequities What they are… Why they are… Where they are… How to address them… Anthony Fleg, UNC volunteer
Goals for the training • Inspiration to work/volunteer to address issues of inequities • Greater understanding of inequities in health • Ability to critically think about the factors behind the scenes that create inequities in health • Ideas for getting involved!
“Of all the forms of inequality, injustice in health care is the most shocking and inhumane…” -Dr. Martin Luther King, Jr.
Addressing discrimination in health care services has been the forgotten frontier of civil rights enforcement...[the government] has lacked the resources, the competence, and the commitment to address disparities in the quality of health services. -Physicians for Human Rights
Obesity rates in women 1988-1994 White Black Mexican Percent of persons obese (BMI>30)
“Eight Americas” • Life expectancy ranges for subgroups of the U.S. population, with Asian women living longest (87.7yrs) and Black/American Indian males living the shortest (66-69yrs) • “Millions of Americans in the most health-disadvantaged groups have life expectancies…similar to some poor developing countries” • Doing best at the ends of the spectrum (children, elderly), but not as well in the young adults and middle-aged
Inequities vs. Inequalities/Disparities
Health Inequalities/Disparities • One group is sicker than another • Unequal distribution of health and disease among populations of people • NIH definition: “Differences in the incidence, prevalence, mortality and burden of diseases and other adverse health conditions that exist among specific population subgroups in the US”. • Note that inequality = disparity = difference in rates of health/disease, without moral/ethical value judgment on this difference
Health Inequities • Health equity = absence of systematic disparities in health (or in the major social determinants of health) between groups with different social advantage/disadvantage (e.g. wealth, power, prestige). -Braveman, Gruskin (2003) • Thus, health inequities are the presence of differences in health and health care, whereby some segments of the population fare better than others.
Health inequality or inequity? Example: the disproportionate numbers of poor and minority citizens in the U.S. that do not have inadequate access to health care • Is it a health inequality? Yes, since there is a difference in rates of access to health care amongst segments of the population • Is it a health inequity? Depends on whether your idea of justice involves “the right to health care”; if so, then yes, it is unfair and unjust that there are differences in this fundamental right, the right to health care • The important difference is that we must make a value judgment in the case of health inequities
A Suggested Framework • Until the recent past, difference in health and disease were not important enough for governments and researchers to study. • This suggests a troubling value judgment that was made for these last centuries – health inequalities are not important enough to study…these inequalities were not considered inequities, and thus, did not deserve attention (for if differences are not unfair differences or unjust differences, then they can be minimized and shrugged off) • Therefore, our default should be to consider every health inequality/disparity as a health inequity, until we can prove that it is not so. • In other words, we should ground our thinking in the human right to health (a value judgment) and therefore treat each and every health inequality/disparity as unfair and unjust until we can prove otherwise.
Components of Health Inequities • Behaviors + cultural practices • Socioeconomic + educational status • Health care delivery • Environmental factors • Communication barriers • Access to health care • “Stress” • Racism/discrimination (real and perceived) • Others?
Three broad categories of causes of inequities in health • Patient factors – behaviors, language barriers, compliance/belief in health system • Institutional factors – policies that discriminate (regardless of intent) • Provider factors – lack of cultural competency, ignorance, bias, stereotyping
A pictorial representation… v o Adapted from V. Hogan
Group case question #1 • A 38 year old man comes to your clinic complaining of polydipsia, polyuria, and feeling “worn out” • Being the smart UNC graduate you are, you do a finger stick and find that his blood sugar is 246, suggestive of diabetes • What factors put a patient at risk for diabetes?
Diabetes (Type 2) • Body develops insulin resistance, with cells not allowing glucose in blood sugar rises • Risk factors -age -obesity -family history -inactivity -diet
Case question #1a • Now, this same patient reveals to you that he is from a Eastern NC community where there is little access to medicine, especially for a farmer like him. He relates to living close to the poverty line, and thinking about going back for his G.E.D. • When asked about diabetes, he looks confused and says, “Isn’t that something to do with sweet blood?” • What additional risk factors does this patient have for diabetes?
Additional risk factors for diabetes • Lack of access to health care • Lack of health insurance • Low level of education • Poverty • Health “illiteracy” • Lack of “health infrastructure” • Unhealthy cultural practices – fried foods, inactivity, etc. • These apply for most chronic disease and are risk factors for poor health in general
Case question 1b • Upon further questioning, the patient relates that his people, the Waccamaw Siouan tribe of Columbus County, are not treated well in the local health system. • In addition, he talks about the traditional belief that diabetes is a form of in-balance that is treatable with a sacred ceremony. • What additional risk factors for diabetes does this information suggest?
American Indians and Diabetes • First, it is important to understand that this group of people suffers disproportionately from the previous lists of risk factors – obesity, health “illiteracy”, poverty, lack of access to health care • Additional risk factors - discrimination (intentional and un-intentional) - trust/belief in the health care system - trust/belief in Western medicine - biological pre-disposition
American Indians and Diabetes • Multiple, additive risk factors for diabetes - 2.5 times more likely to have diabetes - 2.4 times more likely to have diabetes in NC - 4 times more likely to die from diabetes • Question for my colleagues: What might explain the difference between the first two numbers and the third number?
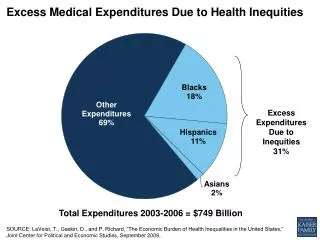
Lots of possible reasons, one of which is that fact that once diagnosed with diabetes and other chronic diseases, many groups do not receive the same level of care as their counterparts…health care is itself a source of inequities.
Health Care Inequities • A big reason why the U.S. ranked 37th in the World Health Organization’s ranking of the world’s health systems! • Present from the beginning of this country, a result of the larger social structure (e.g. those given less rights in society received less health care)
“Discrimination was everywhere, including among the medical and health professionals who furnished care and ultimately determined the structure, design, and operation of the health system.” – S. Rosenbaum
Though the blatant, obvious issues have been addressed, latent institutional and provider factors persist • Before a report in 2002, the medical/health community largely refused to believe that health care inequities existed!
Health care inequities • In one health plan, only 20 percent of African American children with asthma received appropriate follow-up care after an acute episode, compared with 40 percent for Caucasian children. • Filipinos and Native Hawaiians in one health plan had significantly lower rates of breast cancer screening than Caucasians (72% and 75% vs. 81%). • More Hispanics than non-Hispanics with diabetes in one health plan said that their doctors discussed the complications of diabetes with them during all visits (58% vs. 35%). Source: Commonwealth Fund, 2002 publication
Are these examples of health inequalities? Health inequities? • Sickle cell anemia in African Americans • Cystic Fibrosis in Caucasians • Breast cancer in women • Prostate cancer in men
If there is a difference in the rate of disease between groups, there is an inequality in health • The question we must then ask is “Why does this difference exist?” • These are cases of health inequalities due to genetic (sickle cell, CF) and biologic (breast and prostate cancer) differences • These are not necessarily differences that are unfair or unjust, so they would not be health inequities
Genes are a small part of the pie! Adapted from V. Hogan
Question for my colleagues… • If we reduce the rates of disease in the population, will inequities/inequalities in health also lessen?
Life expectancy 1900-1996 Years White Black 1900 1950 1996
Infant Mortality Rates Due to SIDS, United States by race, 1973-1998
Simple answer: NO! • Reducing the difference in disease between groups is much different than reducing the overall rates of disease • Though we have done a great job at making the population healthier, we have not done a great job at lessening the gap between the healthiest and sickest
Health Inequities – Scope? • Example 1: African Americans die from prostate cancer at a rate 2.9 times that of Whites in North Carolina. • Example 2: In 2004, 49-71% of households of recent Latino immigrants had “food insecurity”, compared to 18% of all U.S. households • Example 3: In 2000, life expectancy in Botswana was 33.9 years, compared to 81.6 years in Japan
Worldwide life expectancies (2003) Canada – 80+ years Sub-saharan Africa – 55 years
Scope of Health Inequities • As large and intimidating as the issues are at the local, state, and national level, they are exponentially greater at the global level very little has been done at this point to address the global scope of inequalities in health • Example: In 2006, the vast majority of AIDS patients in the developing world have no access to the anti-retrovirals that have been around for 20 years, drugs to which 100% of AIDS patients in the U.S. have access • The same forces that create inequities in Chapel Hill, Orange county, and North Carolina are at work nationally and globally
Case example #2 • You all have been promoted to the city’s governing board of health (for your awesome work attacking inequalities in your diabetic patients), and are now asked to form 3 “first steps” to address the following statistics, using a $10,000 budget.
Economic and Social Hardships during pregnancy, by ethnicity MIHA, 2002-2003 African American White American < Poverty 44.7 14.9 Hard to make ends meet 22.4 10.7 Food insecurity 19.3 10.4 Food insecurity and hunger 7.3 3.3 No practical support 10.2 6.2 No emotional support 7.2 3.9 Separated or divorced 16.4 4.6 Homeless 7.2 2.3 Involuntary job loss 14.2 6.8 Partner job loss 16.9 11.0 Incarceration of partner 10.5 2.5 Domestic Violence 5.8 1.8 1-5 hardships 70.0 39.0 Source: Braverman P. (Center on Social Disparities in Health, UC-SF)) Presented at Jacobs Institute of Woman’s Health Conference, May 2005
Ideas for the intervention… • Do we focus on the areas of biggest inequities, the areas affecting the largest numbers, or areas that are easiest to address/change? • Focusing on single interventions that would address multiple factors is the best way to turn limited resources (time, funding) into improved health • Interventions that build up the resources of the women (i.e. GED courses, job skills trainings) and are directed with input/advice from the community will be most effective
Case example #3 • I need your help – really! • Issue: As part of the Native Health Initiative’s work, we would like to organize an effort to study the rates of health and disease in the tribes in North Carolina • Why is this data needed? • What would be a first step using a community based participatory research approach? • What barriers/hurdles might we face in collecting this data? • In your groups, brainstorm how you think this project could best be carried out, using the confines of a 1 year time period and an unknown amount of student and tribal support/volunteers.
What to take from tonight: • Get active, stay active! • Commit to learning about issues involved with service with the same vigor as you do for your college coursework! • You may get overwhelmed, and even discouraged at the enormity of the issues remember that all change begins at a micro level, with one-on-one interactions from people who care
Places to serve… • S.H.A.C. (http://www.med.unc.edu/shac/) -volunteer at the clinic or with one of their outreach programs • Native Health Initiative (shameless plug) - www.unc.edu/~flega -summer 2007 internships • Great resources on campus - CCPS, Campus Y, APPLES! • I love to help folks with a specific interest get connected with the organization/project they need – feel free to get in touch! anthony_fleg@med.unc.edu
Places to learn…. • NHI website – www.unc.edu/~flega (click on Library/Links on Health Inequities) • Commonwealth fund – www.cmwf.org • Physicians for Human Rights – www.phrusa.org • North Carolina Office of Minority Health and Health Disparities – www.ncminorityhealth.org • www.improvehealthcare.org
Service and Inequities • You all are the subgroup who sees the need and rewards involved in service work • Motivations of working toward social justice and equality unites service work and work in inequalities • Continue to work/serve for those without voices, without power, without resources…this is our responsibility, as those with voices, power and resources!
We serve life not because it is broken, but because it is holy. -Mother Teresa