Download
1 / 24
250 likes | 663 Vues
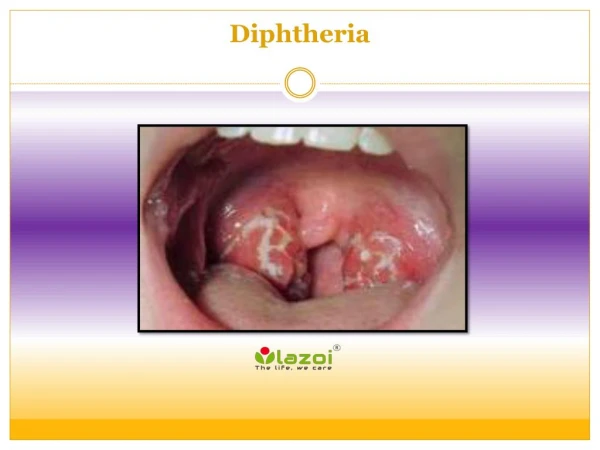
Diphtheria and Pertussis: The Forgotten VPDs. Presented by: Dr Esteghamati National EPI Manager. Challenge. In the context of polio eradication, MMR, MNTE, new vaccines introduction: difficult to raise awareness about old forgotten diseases.

E N D
Diphtheria and Pertussis: The Forgotten VPDs Presented by: Dr Esteghamati National EPI Manager
Challenge In the context of polio eradication, MMR, MNTE, new vaccines introduction: difficult to raise awareness about old forgotten diseases
Current high DTP3(4-5) coverage: changes in epidemiology: shift in age distribution • Low DTP3 coverage countries: outbreaks of diphtheria and pertussis
Diphtheria outbreak IDP camp near Kandahar July – September 2003 Tot Pop: 40,000 10 settlements approx 3000/each 80 cases, 3 deaths CFR 3.8% Since 2002 Number cases Index case 7 24 3 15 6 7 (?) outside cases in neighboring districts 2 deaths (1 in other IDP camp) CFR 29% A 6yo case: wedding in Zare Dasht then infected neighbor x x 9 6 2 5 3
Diphtheria outbreaksEMRO • Yemen 1981-82 • Jordan 1982 • Sudan 1978/1988 • Iraq: suspected outbreak in Sept 2003 • Afghanistan 2002, 2003 • Sporadic cases 1998-2002 in all countries.
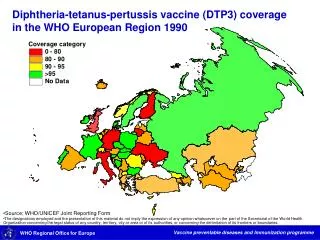
Characteristics of NIS epidemic (Newly Independent States of former Soviet Union) • Largest epidemic in recent years: >150,000 cases and 4500 deaths during 1990-1995 • High proportion of infected adults • Spread from outbreaks in groups with high rates of close contacts (military troops, hospitals, schools,) to a more generalized epidemic, specifically in socio-economically disadvantaged groups
Pakistan: diphtheria fatal case • March 98: 9 yo, resident student of religious school died of diphtheria • School in Islamabad: 400 students 9-20, males • Rapid response: Td vaccination + prophylaxis, and throat swabs from contacts
NIS “scenario” • Large pool of susceptible adults (waning immunity + lack of exposure), coupled with susceptible children, + previous good coverage: potential for epidemic • NIS 0-4 5-9+10-15 >15 (Ukraine) 8% 12% 80% • Iraq (2001-4) 18% 16% 66%
Estimated DTP3 coverage among under one children, EMR, 2002 Palestine 0 0 2 0 33 854 0 10 0 22 2 0 0 0 9 0 0 Bahrain 26 - 90% or more () - 70% - 89% (2) Diphtheria cases reported to WHO, 2002, aggregates 50% - 69% (3) Less than 50% (2)
Pertussis: a challenge! • Major cause of morbidity and mortality: high CFR in dev countries • Highly contagious: rates 2nd transmission in households: 90%, schools 50-80% • Clinical and lab confirmation of B. pertussis is still one of the most difficult challenges facing clinicians • Poor surveillance: disease burden largely unrecognized
Pertussis changing epidemiology in countries with high DTP coverage • In developed countries, with high DTP3 coverage and good surveillance: increase in reported pertussis. • Increase in part due to better recognized cases of pertussis in older adults • In well-immunized populations: shift to older age groups • Older children and adults responsible for transmission of disease to infants and young children
Pertussis in Adults • Accounts for up to 7% of cough illnesses per year • Disease often milder than in infants and children • Adults often source of infection for children
Pertussis Complications Condition Pneumonia SeizuresEncephalopathy Death Hospitalization Percent reported 5.2 0.8 0.1 0.2 20
Clinical case definition A case diagnosed as pertusis by a physician OR A person with a cough lasting at least 2 weeks with at least one of the following • Paroxysm of cough • Inspiratory whooping • Post tussive vomiting
Criteria for lab confirmation • Isolation of bordetella pertusis • Detection of genome sequences by PCR • Rising titer
Reported global DTP3 vaccine coverage and pertussis cases, 1974-2002
Denmark, Finland, UK 2003: Recommendations for preschool aP booster Austria 2003: Recommendation for aP boosters in school-children, adolescents and adults Canada 2003: NACI and CPS recommend aP boosters for adolescents and adults Australia 2003:· Removal of 18-month DTaP dose; switch from Td to TdaP vaccine for 15- to 19-year-olds Some Recent Changes in National Pertussis Immunization Schedules
TdaP Vaccine for Adolescents and Adults: Unanswered Questions • What is the duration of protection? • Will vaccination of adolescents result in decreases in infant pertussis? • Is it necessary to vaccinate additional age groups? If so, how can we do that? • Will pertussis incidence increase in older age groups?
Pertussis surveillance • Difficult clinical diagnosis • Difficult laboratory diagnosis • Poor awareness, poor notification
Estimated DTP3 coverage among under one children, EMR, 2002 Palestine 1 476 1 1439 -(2922) 51 21 27 2 - 233 21 0 8 42 18 96 Bahrain 0 - 213 2 90% or more () - 70% - 89% (2) Pertussis cases reported to WHO, 2002, aggregates 50% - 69% (3) Less than 50% (2)
Disease burden • In most countries, pertussis surveillance inadequate for accurate estimates of cases and deaths • Increased burden of pertussis.
Pertussis (WHO 2000 meeting): Recommendations • Better data for estimating disease burden • Good quality surveillance (case def, age, vacc status, plans for pertussis surveillance) • Outbreaks investigated, reported and documented (guidelines to be developed). • Lab standardization (guidelines for specimen collection, transport, etc) • Monitoring of booster dose policies • Research: develop better understanding of adult disease • Training material to be developed