Download
1 / 13
130 likes | 215 Vues
Collection and analysis of longitudinal pharmacy refill data from manual registers: Experiences from Ugandan public health systems. Joshua Kayiwa INRUD-IAA, Uganda. Session Objectives.

E N D
Collection and analysis of longitudinal pharmacy refill data from manual registers: Experiences from Ugandan public health systems Joshua Kayiwa INRUD-IAA, Uganda
Session Objectives • Narrate the experience of the Uganda INRUD-IAA team in collecting, cleaning, summarizing and analyzing manually recorded pharmacy refill data for longitudinal research • Make recommendations for similar longitudinal studies in the African health systems context
Brief Background • Most public health systems in low and middle income countries maintain patients’ treatment data in manual registers • Mainly due to constraints in technological, financial and human resource capacity to design and maintain appropriate Electronic Medical Record Systems (EMRs) • Has implications for data security, availability, accessibility, accuracy, completeness, and the ease of using such data to study policy impacts
Background to INRUD-IAA Study • Designed as a longitudinal staggered entry interventional study among six public health facilities in Uganda • Aim was to investigate the extent to which low-cost interventions meant to reduce clinic congestion, implemented at health facility level would improve patients’ individual-level adherence to antiretroviral therapy (ART) • Results in press and also presented elsewhere in this ICIUM meeting • Collected pharmacy-refill information for evaluation • Appointment dates, actual visit dates, numbers of pills dispensed • 720 ART-experienced and 761 patients newly initiating ART for six months pre-intervention and nine months post-intervention
Where Were Raw Data Found? • Longitudinal patient-level data in clinical records, diaries, pharmacy, appointment registers • Manually filled and kept at facility or with patients
What Were We Trying to Measure? Key study outcomes : • % of experienced patients with >30 days of dispensed medication • % of experienced patients missing any scheduled visit • % of experienced patients with 3 or more days without medication • Time until newly-treated patients experienced a medication gap of >7 or >14 days during first 120 days of treatment
Challenges with Collecting Data from Manual Registers and Diaries • Data availability • Health workers only record what they think they need to administer today’s treatment • Data often missing, e.g., # of pills dispensed, patients’ CD4 and viral load history • Data accessibility and security • Hard to access, especially for patient diaries • Diaries prone to wear and tear due to mishandling • Pages may tear out or be destroyed by cockroaches / mould • Data accuracy and reliability • Data not protected against entry errors • Cannot be verified against secondary sources.
Managing Longitudinal Data Collected from Manual Registers • Data collected and recorded using a standard tool by trained research assistants • Data entry and validation • Customized double entry data input and validation using MS Excel • Further quality checks in Stata before analysis
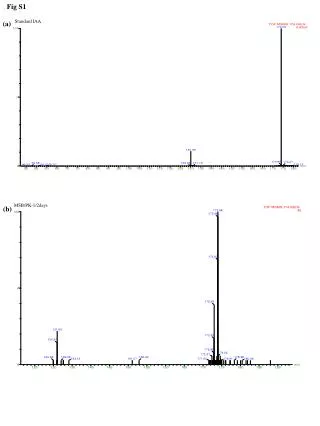
Summarizing the Data • Using appointment and visit dates and days of medication dispensed, we computed: • % of patients receiving more than 30 days of medication • Number of days by which patient missed any visit (see graph) • Gaps medication availability between appointments
Key Findings (manuscript in press) • Among experienced patients, interventions led to • Significant two-fold increase in patients receiving >30 days of dispensed medication • Significant 33% reductions of missed appointments • Significant 31% reductions of experiencing a medication gap of 3+ days • Among newly treated patients, interventions associated with • Significant 44% reduction in hazard of experiencing medication gap of >7 days (see graph) • Significant 38% reduction medication gap of >14 days
Aim Achieved? • We aimed to determine whether interventions to reduce clinic congestion, improve patient flow and if this would translate into better ART adherence. • Using routine data from manual clinic records, we were able to measure increases in days of medication dispensed, reductions in missed visits, and fewer medication gaps among ART patients.
Lessons Learnt and Recommendations • It is possible to collect pharmacy refill records from manual registers in African health facilities • Many challenges: especially data completeness, accuracy, security and reliability • Recommendations • Manual pharmacy registers and clinical records safer when kept at the health facility than with patients • More attention to staff training in record keeping • Unless staff see data used for clinical care, management, or research, they have no incentive to record accurately • Pharmacy refill records should ideally be kept electronically, whenever resources (human and financial) allow