Download
1 / 79
790 likes | 930 Vues
Tony Tommasello, Ph.D. University of Maryland School of Pharmacy Office of Substance Abuse Studies 410 706-7513 atommase@rx.umaryland.edu. Controlled Substance Management or “Doctor I need Oxy”. Program Objectives. At the end of this program participants will be better able to:

E N D
Tony Tommasello, Ph.D. University of Maryland School of Pharmacy Office of Substance Abuse Studies 410 706-7513 atommase@rx.umaryland.edu Controlled Substance Management or“Doctor I need Oxy”
Program Objectives • At the end of this program participants will be better able to: • Screen for substance abuse • Assess the severity of a patient’s involvement with alcohol or illicit drugs • Determine the legitimacy of a patient’s request for opioid analgesics • Justify and document the decision to prescribe or refuse to prescribe CDS
Lawnmower Addict L.A. is a 42 Y.O. male who broke his ankle while mowing wet grass across an incline. After several surgical attempts including failed pinning operations, his foot is rotated 60 degrees out of alignment and he has chronic pain. Prior to this injury L.A. had a history of opioid addiction. He states that he is committed to recovery and participates in 12-step N.A. meetings but he abused his last oxycodone prescription and experienced a relapse. His goal is to achieve pain relief without relapse to opioid abuse.
Enduring pain to avoid relapse E.P. is a 40 y.o. married male with 4 children, He has been in opioid addiction recovery for over 9 years. I received a tearful midnight call from his wife stating the E.P. was lying in bed in a fetal position, moaning in pain and refusing to take opioid analgesics after incurring a back injury while wrestling with his son who is a star member of the high school wrestling team. His goal is to never relapse to active opioid addiction.
Scope of the Public Health Problem • An estimated 2.4 million people have used heroin at some time in their lives (NHSDA, 1998) • During 1996 through 1998, an estimated 471,000 persons used heroin for the first time. Of them, 25% were under age 18 and another 47% were age 18 - 25 (NHSDA, 1999)
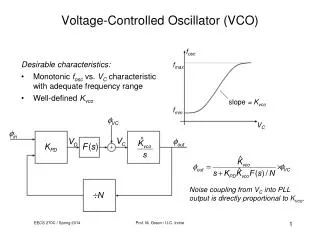
Heroin Price Falls, Purity Increases1980 through 1998 Purity (% heroin) Purity (% heroin) Price in $US Price in $US Data from U.S. Department of Justice: Drug Enforcement Administration
What about abuse? • According to the National Institute on Drug Abuse (NIDA), in 1999 Four million Americans reported current use of prescription drugs for non-medical purposes • The most dramatic increases were found among the 12 to 25 year olds • Oxycontin® and Ritalin® were among the most cited abused medications
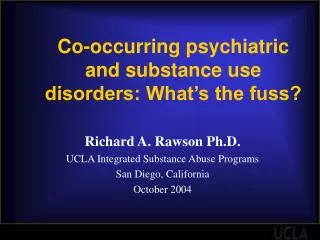
Number of U.S. Narcotic Analgesic-Related ED Visits, 1994-2001 Source: www.samhsa.gov/oas/2k3/pain/dawnpain.pdf
Narcotic Abuse Taxes ED Resources • In 2001 there were an estimated 90,232 ED visits, a 117% increase since 1994 • “Dependence” was the most frequently mentioned motive for abuse (44% of cases) • Between 2000 and 2001 Oxycodone mentions increased 70% and accounted for 53.7% of the overall increase in narcotic abuse cases during that year. Source: The DAWN report January 2003. http://www.samhsa.gov/oas/2k3/pain/DAWNpain.pdf
Teen Abuse of Rx DrugsNational figures Curran JJ: Prescription for Disaster – The growing problem of prescription drug abuse in Maryland. Sept 2005.
Access to treatment is limited • Of the estimated 810,000 opioid dependent persons in the U.S. only 170,000 maintenance treatment slots exist.
Therapeutic drug use: • Drug use to treat or diagnose illness. Almost everyone has taken a drug at one time or another because they were sick. • A direct and reliable drug effect is expected. Antibiotics kill bacteria regardless of the sick person’s belief in the medicine. The drug is a known entity. • There are rules. The prescription tells: what to take, how much to take, and when to take it. A person who violates the rules must own the consequences.
Social Drug Use • Drugs are used to increase social interactions. • Rules are vague or non-existent. • Drug supply is uncertain • Most cases of addiction result from social drug use that gets out of control.
A Basic Distinction • High seeking = Pain relief seeking • “Because 6 to 15% of the U.S. population abuses drugs, the history of pain management is marked by the undertreatment [of pain in] the other 85 to 94%.” Passik SD quoted in:Gilson AM and Joranson DE (2002) U.S. Policies Relevant to the Prescribing of Opioid Analgesics for the Treatment of Pain in Patients with Addiction Disease Clinical Journal of Pain 18:S91-S98. available at http://www.medsch.wisc.edu/painpolicy/
Pain Statistics • Most common reason that people seek medical care • 50 million Americans are partially or totally disabled due to pain • Annual cost to U.S. society estimated to exceed $100 billion • 50-80% of patients with pain report that their pain is inadequately managed • Risk of undertreatment is increased among those with a history of substance abuse
Addiction Defined • Addiction is compulsive use with loss of control and continued use despite adverse consequences.
Elements of Compulsivity: • Constant thought of drug acquisition • Anticipation of opportunities to use • Defer other priorities of life • Unable to resist desire to use
Aspects of Loss of Control • Inability to use in moderation consistently • Easier to abstain completely • Frequent episodes of excessive use
Continued use despite problems • Loss associated with use • Multiple crisis not seen as drug-related • Sincere promises to self and others to quit
Signs of Psychological Dependence • Carrying Drugs • Using Drugs alone • Stockpiling Drugs • Concern over supply • Changing friends • Finding excuses to use • Using at inappropriate times • Willingness to take increasing risks
The Memory of Drugs Amygdalanot lit up Amygdalaactivated Front of Brain Back of Brain Nature Video Cocaine Video
DSM IV: Substance Dependence • 3 of following in 12 month period: • Tolerance • Withdrawal • Difficulty cutting down (loss of control) • Time spent drug seeking (compulsive use) • Decrease in activities • Continued use despite knowledge of persistent physical or psychological problems
Addiction Characteristics • First priority is drug acquisition and use • Negative consequences occur in order • 1) Interpersonal relationships suffer • 2) Productivity declines • 3) Self-Esteem plummets • 4) Health problems emerge or worsen • Note: Legal problems can occur at any time.
Why Treatment ? Rewards • Dysfunctional lifestyle of opioid addiction makes treatment a desired alternative • Oral methadone and buprenorphine sublingual tablets are approved for both medical withdrawal and medical maintenance Negative consequences Utility Theory
Addictive Behaviors • Selling prescription drugs • Prescription forgery • Stealing drug from others • Injecting oral formulations • Buying drugs on the street • Resistance to change therapy despite evidence of adverse effects from the drug
Pseudo-addiction • Drug-seeking behavior misidentified by health providers as addictive behavior, when it is actually relief-seeking behavior • Behaviors resembling those of drug addiction disappear when patient is given adequate doses of analgesia
Pseudoaddiction Behaviors • Complaints for more drug • Hoarding drug during pain free periods • Specific drug requests • Openly seeking other sources of help • Occasional unsanctioned dose increases • Resistance to change in therapy
Principles Physical Dependence = Addiction Pain Management with opioids Addiction (<3%)* Physical dependence (common) * Brushwood et al. (2002) Pharmacists’ Responsibilities in Manageing Opioids: A Resource APhA Special Report American Pharmacists Association.
SummaryDifferentiating factors • Motivation for use • Route of administration • Frequency of use and dose • Pseudo-addiction? • Continued use despite problems
Types of Pain • Nociceptive • Pain resulting from actual or potential tissue damage • Results from ongoing activation of primary afferent nociceptive neurons by noxious stimuli • Neuropathic • Results from a disturbance in function or pathologic change in a neuron • Can be peripheral or central
Non-Verbal Signs of Pain • Aggressive behavior • Changes in daily activities • Facial expression • Bodily movements • Vocal • Mood • Physical Assessment Values • Change in vital signs
Symptom Analysis • Precipitating events • Palliating events • Quality • Severity • Pain location and radiation • Temporal relationships • Associated symptoms • Previous treatments and their effects
Pain Scales Numerical Pain Scale Faces Pain Scale
Pain Assessment • Accept the patient’s description • Thorough assessment of each pain • History, examination, investigation • Assess impact of pain on ADLs and functional status • Assess other factors that influence pain • Physical, psychological, social, cultural, spiritual • Reassessment
WHO-Step Ladder Severe Morphine Hydromorphone Methadone Levorphanol Fentanyl Oxycodone ± Adjuvants Moderate APAP/Codeine APAP/Hydrocodone APAP/Oxycodone APAP/Dihydrocodeine Tramadol ± Adjuvants Mild Aspirin Acetaminophen NSAIDs ± Adjuvants Adapted from: World Health Organization. Cancer Pain Relief. 1996.
Patient Centered Treatment Goals • “What would you like to do that you can’t do because of your pain?” • “I’d like to be able to do my needlework” • “I’d like to walk to the bathroom – alone” • “I want to sleep through the night” • “I want to go back to work” • “I want to be able to play with my children”
With Uncontrolled Pain … Emotional Effects Depression, anxiety, anger Cognitive Effects Somatic focus, helplessness, “catastrophization” Behavioral Effects Inacitvity, social/sexual dysfunction, poor sleep, loss of productivity Physical Changes Muscle tension, poor posture, circulatory impairment, obesity Increased PAIN and Dysfunction PAIN
No History of Abuse (Group 1)* Substance abuser in the past (Group 2)* Addict in recovery including opioid maintenance patient Active substance abuser (Group 3)* Nociceptive pain Acute Chronic Somatic Visceral Neuropathic pain Chronic Acute Four kinds of patientsTwo kinds of pain * Gourlay et al. (2005) Pain Medicine 6(2) 107-112
The CAGE Screen • Have you ever felt the need to Cut Down on your drinking • Have you ever been Annoyed by criticism of your drinking • Have you ever felt Guilty about your drinking • Have you ever needed an Eye Opener to get going in the morning.
Toxicology Screening Tests Qualitative results Purposes • To identify surreptitious use • To monitor known users Clinical Examples • Prenatal Care • Impaired Professionals • Trauma/ER
Legitimate patient with no Hx of addiction (Group 1*) • Manage pain (analgesic ladder) • Recognize low addiction risk • Differentiate physical dependence from addiction • Don’t mistake pain relief seeking for drug seeking - pseudoaddiction * Gourlay DL et al. (2005) Universal precautions in pain medicine: A rational approach to the treatment of chronic pain. Pain Medicine 6(2), 107-112.
Pain Management and Addiction Confusion over the distinction between physical dependence (a state of adaptation that produces withdrawal signs upon abrupt drug discontinuation) and addiction (DSM-IV Substance Dependence) has confounded approaches to the patient in pain.
Misconception regarding pain management with opioids • Misconception: Therapeutic use of opioids is commonly associated with substance abuse or addiction • Reality: In patients with no history of substance abuse the risk of addiction following therapeutic use appears to be less than 3%
Clinical Features Distinguishing Opioid Use in Patients With Pain Versus Patients Who Are Addicted to Opioids (TIP 40)
Patient populations under-treated for pain • Elderly • Minorities • Children • Terminally ill patients with HIV/AIDS • Chronic non-cancer pain • Perceived as high addiction risk • Gilson AM and Joranson DE (2002) U.S. Policies Relevant to the Prescribing of Opioid Analgesics for the Treatment of Pain in Patients with Addiction Disease Clinical Journal of Pain 18:S91-S98. available at http://www.medsch.wisc.edu/painpolicy/
Addict in solid recovery (Group 2*) • May refuse adequate pain pharmacotherapy • Use of buprenorphine • Suggest increased support group work while on analgesic pharmacotherapy • Conduct urine or saliva screens for unauthorized substances • Utilize pain management contract * Gourlay DL et al. (2005) Universal precautions in pain medicine: A rational approach to the treatment of chronic pain. Pain Medicine 6(2), 107-112.