Download
1 / 1
10 likes | 119 Vues
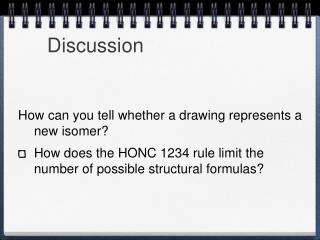
Post Extubation Airway Obstruction from Occult Laryngeal Mass R. Scott Childs, MD, J. Rivera-Melendez, MD, N. N. Knezevic , MD, PhD, K. D. Candido , MD Department of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA. Abstract. Case Description.

E N D
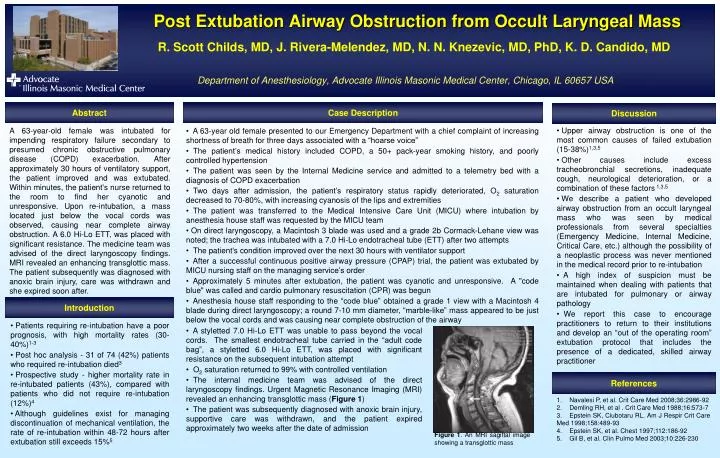
Post Extubation Airway Obstruction from Occult Laryngeal MassR. Scott Childs, MD, J. Rivera-Melendez, MD, N. N. Knezevic, MD, PhD, K. D. Candido, MDDepartment of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA Abstract Case Description Discussion • Upper airway obstruction is one of the most common causes of failed extubation (15-38%)1,3,5 • Other causes include excess tracheobronchial secretions, inadequate cough, neurological deterioration, or a combination of these factors 1,3,5 • We describe a patient who developed airway obstruction from an occult laryngeal mass who was seen by medical professionals from several specialties (Emergency Medicine, Internal Medicine, Critical Care, etc.) although the possibility of a neoplastic process was never mentioned in the medical record prior to re-intubation • A high index of suspicion must be maintained when dealing with patients that are intubated for pulmonary or airway pathology • We report this case to encourage practitioners to return to their institutions and develop an “out of the operating room” extubation protocol that includes the presence of a dedicated, skilled airway practitioner A 63-year-old female was intubated for impending respiratory failure secondary to presumed chronic obstructive pulmonary disease (COPD) exacerbation. After approximately 30 hours of ventilatory support, the patient improved and was extubated. Within minutes, the patient's nurse returned to the room to find her cyanotic and unresponsive. Upon re-intubation, a mass located just below the vocal cords was observed, causing near complete airway obstruction. A 6.0 Hi-Lo ETT, was placed with significant resistance. The medicine team was advised of the direct laryngoscopy findings. MRI revealed an enhancing transglottic mass. The patient subsequently was diagnosed with anoxic brain injury, care was withdrawn and she expired soon after. • A 63-year old female presented to our Emergency Department with a chief complaint of increasing shortness of breath for three days associated with a “hoarse voice” • The patient’s medical history included COPD, a 50+ pack-year smoking history, and poorly controlled hypertension • The patient was seen by the Internal Medicine service and admitted to a telemetry bed with a diagnosis of COPD exacerbation • Two days after admission, the patient’s respiratory status rapidly deteriorated, O2 saturation decreased to 70-80%, with increasing cyanosis of the lips and extremities • The patient was transferred to the Medical Intensive Care Unit (MICU) where intubation by anesthesia house staff was requested by the MICU team • On direct laryngoscopy, a Macintosh 3 blade was used and a grade 2b Cormack-Lehane view was noted; the trachea was intubated with a 7.0 Hi-Lo endotracheal tube (ETT) after two attempts • The patient's condition improved over the next 30 hours with ventilator support • After a successful continuous positive airway pressure (CPAP) trial, the patient was extubated by MICU nursing staff on the managing service’s order • Approximately 5 minutes after extubation, the patient was cyanotic and unresponsive. A "code blue" was called and cardio pulmonary resuscitation (CPR) was begun • Anesthesia house staff responding to the “code blue” obtained a grade 1 view with a Macintosh 4 blade during direct laryngoscopy; a round 7-10 mm diameter, “marble-like” mass appeared to be just below the vocal cords and was causing near complete obstruction of the airway Introduction • Patients requiring re-intubation have a poor prognosis, with high mortality rates (30-40%)1-3 • Post hoc analysis - 31 of 74 (42%) patients who required re-intubation died3 • Prospective study - higher mortality rate in re-intubated patients (43%), compared with patients who did not require re-intubation (12%)4 • Although guidelines exist for managing discontinuation of mechanical ventilation, the rate of re-intubation within 48-72 hours after extubation still exceeds 15%5 • A styletted 7.0 Hi-Lo ETT was unable to pass beyond the vocal cords. The smallest endotracheal tube carried in the “adult code bag”, a styletted 6.0 Hi-Lo ETT, was placed with significant resistance on the subsequent intubation attempt • O2 saturation returned to 99% with controlled ventilation • The internal medicine team was advised of the direct laryngoscopy findings. Urgent Magnetic Resonance Imaging (MRI) revealed an enhancing transglottic mass (Figure 1) • The patient was subsequently diagnosed with anoxic brain injury, supportive care was withdrawn, and the patient expired approximately two weeks after the date of admission References 1. Navalesi P, et al. Crit Care Med 2008;36:2986-92 2. Demling RH, et al . Crit Care Med 1988;16:573-7 3. Epstein SK, Ciubotaru RL. Am J Respir Crit Care Med 1998;158:489-93 4. Epstein SK, et al. Chest 1997;112:186-92 5. Gil B, et al. Clin Pulmo Med 2003;10:226-230 Figure 1. An MRI sagittal image showing a transglottic mass