Download
1 / 18
180 likes | 222 Vues
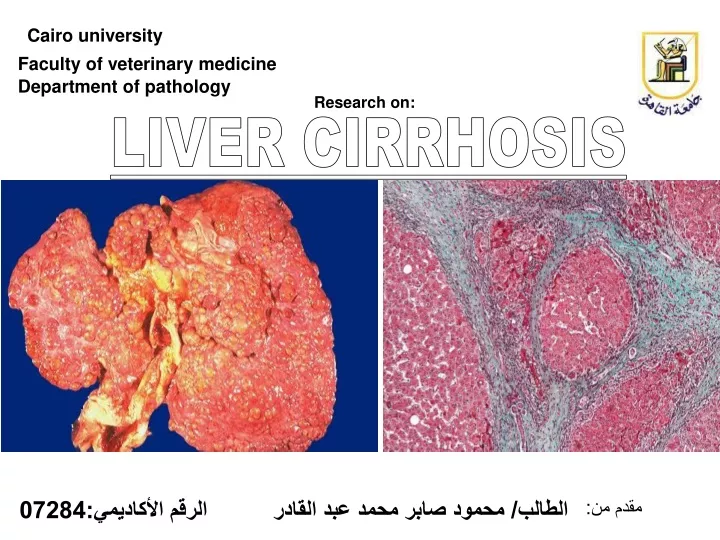
Cairo university. Faculty of veterinary medicine. Department of pathology. Research on:. LIVER CIRRHOSIS. الطالب/ محمود صابر محمد عبد القادر الرقم الأكاديمي:07284. مقدم من:. CONTENTS. Introduction Definition & Etiology Common Symptoms of Cirrhosis Pathophysiology

E N D
Cairo university Faculty of veterinary medicine Department of pathology Research on: LIVER CIRRHOSIS الطالب/ محمود صابر محمد عبد القادر الرقم الأكاديمي:07284 مقدم من:
CONTENTS Introduction Definition & Etiology Common Symptoms of Cirrhosis Pathophysiology PATHOLOGY ,Pathogenesis& Classification MORPHOLOGY OF CIRRHOSIS EVOLUTION OF CIRRHOSIS ACTIVITY OF CIRRHOSIS REFERENCES
Introduction Cirrhosis is a consequence of chronic liver disease characterized by replacement of liver tissue by fibrosis, scar tissue and regenerative nodules (lumps that occur as a result of a process in which damaged tissue is regenerated), leading to loss of liver function. Cirrhosis is most commonly caused by alcoholism, hepatitis B and C, and fatty liver disease but has many other possible causes. Some cases are idiopathic, i.e., of unknown cause. Ascites (fluid retention in the abdominal cavity) is the most common complication of cirrhosis and is associated with a poor quality of life, increased risk of infection, and a poor long-term outcome. Other potentially life-threatening complications are hepatic encephalopathy (confusion and coma) and bleeding from esophageal varices. Cirrhosis is generally irreversible, and treatment usually focuses on preventing progression and complications. In advanced stages of cirrhosis the only option is a liver transplant. The word "cirrhosis" derives from Greek κίρῥος, meaning tawny (the orange-yellow colour of the diseased liver). While the clinical entity was known before, it was René Laennec who gave it the name "cirrhosis" in his 1819 work in which he also describes the stethoscope Normal Liver CIRRHOSIS
Definition & Etiology Cirrhosis is a common chronic, progressive and diffusive liver disease, caused by one or several agents act repeatedly and persistently. Histologically, cirrhosis is an irreversible alteration of the liver architecture, consisting of hepatic fibrosis and areas of nodular regeneration In other words, It is a Diffuse fibrosis of the liver with nodule formation. or Abnormal response of the liver to any chronic injury Causes of Cirrhosis: Chronic viral hepatitis & Prolonged cholestasis (primary biliary cirrhosis, primary sclerosing cholangitis)& Autoimmune diseases (autoimmune hepatitis) Drugs and toxins & Alcohol& Certain parasitic infections (such as schistosomiasis) Normal Liver CIRRHOSIS
Common Symptoms of Cirrhosis Jaundice (Yellow skin or eyes) Ascites (Fluid in abdomen) Hepatomegaly (Enlarged liver) Edema (Swelling of the legs, feet, and back) Fatigue and weakness Loss of appetite Weight loss and nausea Whole body itching (pruritis) Mental confusion Redness of the palms of the hands Small, red spider-like vessels Decreased urine output Pale or clay colored stools Vomiting blood (portal hypertension) Nosebleeds
normal cirrhotic Pathophysiology The liver plays a vital role in synthesis of proteins (e.g., albumin, clotting factors and complement), &detoxification and storage (e.g., vitamin A). In addition, it participates in the metabolism of lipids and carbohydrates. Cirrhosis is often preceded by hepatitis and fatty liver (steatosis), independent of the cause. If the cause is removed at this stage, the changes are still fully reversible The pathological hallmark of cirrhosis is the development of scar tissue that replaces normal parenchyma, blocking the portal flow of blood through the organ and disturbing normal function. Recent research shows the pivotal role of stellate cell, a cell type that normally stores vitamin A, in the development of cirrhosis. Damage to the hepatic parenchyma leads to activation of the stellate cell, which becomes contractile (called myofibroblast) and obstructs blood flow in the circulation. In addition, it secretes TGF-β1, which leads to a fibrotic response and proliferation of connective tissue. Furthermore, it disturbs the balance between matrix metalloproteinases and the naturally occurring inhibitors (TIMP 1 and 2), leading to matrix breakdown and replacement by connective tissue-secreted matrix.[8] The fibrous tissue bands (septa) separate hepatocyte nodules, which eventually replace the entire liver architecture, leading to decreased blood flow throughout. The spleen becomes congested, which leads to hypersplenism and increased sequestration of platelets. Portal hypertension is responsible for most severe complications of cirrhosis. Showing cirrhosis Micrograph Trichrome stain
PATHOLOGY ,Pathogenesis& Classification the first theory as to the pathogenesis of this disorder was advanced by Roessle: parenchymal degeneration, regeneration and scarring which is now understood according to the following sequence: INJURYDEGENERATIONFIBROSISFORMATION OF FIBRO-VASCULAR MEMBRANESPARENCHYMAL DISSECTION INTO NODULESREARRANGEMENT OF BLOOD CIRCULATIONCIRRHOSIS which is considered by most experts as a self-perpetuating irreversible process. Regenerative nodules may form in the fibrous septa but they are not necessary for the histological diagnosis of cirrhosis: as nodules alone without fibrosis do not constitute cirrhosis. In this disease, the nodularity of the liver is mostly the result of fibrosis dissecting the parenchyma in small uniform acinar or subacinar nodules in micronodular types and in lobular and plurilobular large non-uniform nodules in macronodular forms. Regenerative nodules develop in the midst of scars but are a late phenomenon. They are important, however, for the advancement and neoplastic transformation of the cirrhosis. According to World Health Organization :it classified according to: MORPHOLOGIC: Macronodular & Micronodular & Mixed HISTOLOGIC: Portal, Post-necrotic, Post Hepatitic, Biliary, Congestive ETIOLOGIC AGENTS: Genetic, Toxic, Infectious, Biliary, Vascular, Cryptogenic
MORPHOLOGY OF CIRRHOSIS GROSS INSPECTIONGrossly, with the naked eye, a cirrhotic liver appears nodular, "hub-nailed", on the external surface and nodular on the cut surface. Variation in size, color, shape and consistency is relevant and may help in the identification of the etiology. The liver is usually indurated shrunken and yellowish-tan but it may be enlarged and yellow as in alcoholic fatty cirrhosis, rusty as in hemochromatosis or large and green as in biliary obstruction. It is usually the privilege of the surgeon to inspect the liver in vivo, therefore he must acquaint himself with the gross changes of cirrhosis and develop the ability of detecting discolorations of possible neoplastic nodules in order to obtain adequate samples for histological examination MACRONODULAR CIRRHOSIS: Larger nodules separated by wider scars and irregularly distributed throughout the liver usually due to an infectious agent such as viral hepatitis which does not diffuse uniformly throughout the liver MICRONDULAR CIRRHOSIS: Small rather uniform 2m nodules seperated by thin fibroussepta usually due to a chemicalagent as alcohol which diffuseuniformly throught the liver.
MICROSCOPIC CHANGES Presence of nodules and fibrous septa with effacement of the lobular architecture. The nodules are of two types: Dissection type and Hyperplastic Regenerative type DISSECTION NODULES contain remnants of portal tracts and central veins. are separated by wide scars but contain thin fibrous septa. contain dilated sinusoids especially at their periphery looking like multiple central veins obviously produced by the inflow of arterial blood coming from the surrounding wide scars. the portal tracts within large nodules may be hypoplastic containing portal venule and arteriole but no bile ducts giving the impression of a disappearing bile duct disorder.. within wide scars regenerative nodules may develop..
HYPOPLASTIC PORTAL FIELD: In a dissecting nodule. Notice presence of portal vein, portal artery but no bile duct.This case was interpreted as "vanishing duct syndrome" REGENERATIVE NODULES these occur in micro and macro nodular cirrhosis they arise in the midst of scars favored by the rich arterial blood of scar tissue they are round nodules with a fibrous pseudo capsule with bile ductules due to obstruction of bile flowthey have embryonal type of cell plates, two cells thick, "twinning of cell plates" nuclei are aligned at the sinusoidal pole of the plates they often show focal cholestasis they may undergo dysplastic and malignant changes they compress the vessels of the capsule contributing to the perpetuation of the cirrhosis
THE FIBROUS SEPTA: Are, with nodules, the other characteristic component of cirrhosis and they are visible even with the naked eye. They have been termed "fibro-vascular membranes" which provide a diversion of the blood flow through an alternative route along these fibrous septa instead of through the acinar sinusoids, thus affecting the physiology of the hepatocytes The fibrous septa are basically granulation tissue more or less active according to the degree of edema, capillarization, inflammatory cell infiltration and fibrosis. They reflect the activity of the cirrhotic process ACTIVE SEPTA Thick connective tissue bands containing edema, many chronic inflammatory cells and irregular demarcation with the parenchymal liver tissue PASSIVE SEPTA Slender connective tissue bands containing few chronic inflammatory cells and sharp demarcation with parenchymal liver tissue
EVOLUTION OF CIRRHOSIS The evolution can be assessed on degree of fibrosis and nodule formation. The following stages can be identified with some approximation even on a needle biopsy specimen 1-INCOMPLETE SEPTAL(Incomplete bridging fibrosis, no nodules) EARLY2-(Thin bridging fibrosis with dissecting nodules) MODERATELY ADVANCED3-(Thick bridging fibrosis with dissecting nodules) 4-ADVANCED(Wide septa with regenerative hyperplastic nodules)
ADVANCED CIRRHOSIS: Wide scars containing clusters of regenerative hepatocytes. Large scars may contain large portal fields recognizable with a stain for elastic fibers EARLY CIRRHOSIS: Thin fibrous septa with dissecting nodules. No regenerative nodules. Presence of multiple efferent vessles. (Reticulim stain by silver impregnation INCOMPLETE SEPTAL CIRRHOSIS: Presence of very slender septa radiating from enlarged fields toward the center of the lobule. There are distended efferent vessels around the septum. This type of cirrhosis produces only portal hypertension and no liver failure. The prognosis is very good if the portal hypertension is controlled
ACTIVITY OF CIRRHOSIS Activity is assessed by extent of cell damage, inflammatory reaction within the scar tissue, piecemeal necrosis along fibrous septa, edema of the septa and changes in the parenchymal nodules such as necrosis and cholestasis. Activity indicates the progression of the cirrhotic process and is graded as: INACTIVENo inflammation and intact limiting plates around septa which are fibrotic SLIGHTMild inflammation; segmental erosion of limiting plates MODERATEModerate inflammation and damage of limiting plates SEVEREMarked inflammation, extensive damage of limiting plates, piecemeal necrosisand parenchymal damage, i.e.: necrosis, cholestasis, dysplasia, malignant transformation
COMPLICATIONS OF CIRRHOSIS About one third of cirrhosis are compensated and, do not produce any clinical symptoms and are accidentally discovered during a medical examination or an operation or at autopsy. The rest are decompensated and produce complications mainly due to liver failure and portal hypertension. They are: ASCITES VARICESEsophageal varices, hemorrhoids PORTAL VEIN THROMBOSISDIGESTIVE HEMORRHAGES JAUNDICE HEPATIC ENCEPHALOPATHY IMPAIRED COAGULATIONANEMIA INFECTION INFARCTION OF NODULES MALIGNANT CHANGE (HEPATOCELLULAR CARCINOMA) IN NODULES
MALIGNANT TRANSFORMATION: of a regenerative nodule. Notice the capsule, the peripheral zone of the regenerative nodule and the inner zone of hepatocellular carcinoma. HEPATIC ENCEPHALOPATHY
REFERENCES Lectures on veterinary pathology (353) WEB SITES: www. epcity.com www.meddean.luc.edu/lumen/MedEd/orfpath/cirhosis.htm www.en.wikipedia.org