Download
1 / 25
260 likes | 438 Vues
SMC . Scottish Antimicrobial Prescribing Group [SAPG] A National Stewardship Programme: SAPG and Acute Medicine . Dilip Nathwani Chair of SAPG . Why antibiotic prescribing and infection management?. Antimicrobial Prescribing Facts: Rule of “1/3”.

E N D
SMC Scottish Antimicrobial Prescribing Group [SAPG] A National Stewardship Programme: SAPG and Acute Medicine Dilip Nathwani Chair of SAPG
Antimicrobial Prescribing Facts: Rule of “1/3” ~ 1/3 of all hospitalised inpatients at any given time receive antibiotics ~ up to 1/3 to ½ are inappropriate ~ up to 30% of all surgical prophylaxis in inappropriate ~ 30% of hospital pharmacy budgets. Stewardship programmes can save up to 10-30% of pharmacy budgets. 30% of hospital patients are on antibiotics Of these, 30% are prescribed because of HAI: importance of Infection control
Risk of resistance to the individual ~ 2 fold for 2 months and up to 12 months1 ~8- 10 fold risk of CDAD up to 3 months2 AGE Co-morbidity Type of antibiotic (~8 fold with cephalsporins and 30 fold with quinolones) “Price of an antibiotic” • 1BMJ 2010; 340: 1120; • 2CMI 2009; 15:427-434
31 hospitals 27.8% patients on antimicrobials 50.5% given intravenously 76.1% reason recorded in case notes 57.9% compliant with local guidelines 30.3% surgical prophylaxis more than one day some room for improvement! Current landscape of hospital antibiotic prescribing in Scotland: National Survey June 2009
RESTRICTED ANTIBIOTICS AND IMPACT ON CDAD AND MRSA: UK EVIDENCE • Large UK [London] hospital • CDI increasing • Restricted narrow spectrum antibiotic intervention • ITS analysis • Reduction in rates of CDI and MRSA • No change in mortality
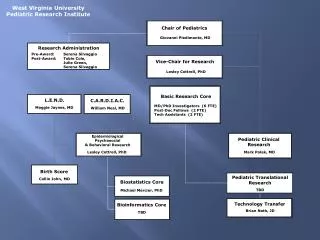
What is SAPG? • Multidisciplinary national clinical forum based on SMC collaborative structure • Staffed by Project Lead (pharmacist), Project Officer & Information Analyst • Includes representatives from key national stakeholders - SMC, QIS, ISD, HPS, NES and SGHD and all mainland NHS boards.
Antimicrobial Management Team (AMT) • Sub-group of NHS Board Area Drug & Therapeutics Committee • Key role in progressing SAPG work at local level • Lead doctor, Consultant Microbiologist, Antimicrobial Pharmacist, Infection Control Manager, Primary Care representative
Chief Executive Infection Control Manager Medical Director Area Drugs & Therapeutics Committee Risk Management Committee ANTIMICROBIAL MANAGEMENT TEAM (AMT) Clinical Governance Committee Dissemination& feedback Infection Control Committee Antimicrobial Pharmacist Microbiologist / Infectious Diseases Physician Prescribing support / feedback Ward Based Clinical Pharmacists PRESCRIBER
Aim:Scottish Antimicrobial Prescribing Group (SAPG) • Improve the quality of antimicrobial prescribing and infection management in hospitals and primary care • Reduce amount and reduce broad spectrum • Improve quality of prescribing [choice, route, dose, duration, timeliness] • Reduce harm (mortality, CDAD, resistance) • Measure improvement • Measure unintended harm (complications e.g nephrotoxicity and ototoxicity, readmissions, increased ICU referral, resistance, other)
WORKSTREAMS • Organisation and Accountability -Structures, Leadership, Performance targets • National and Local Information • Antimicrobial Surveillance • Antibiotic Consumption • Dissemination and sharing of data • Education • Multi-professional • Team based • Infection management • Protocols, Community acquired Pneumonia Improvement, acute care infection management • Care Homes
HIGH IMPACT INFECTIONS IN ACUTE MEDICINE • Pneumonia/LRTI’s • Infective exacerbation of COPD • UTI • Skin and soft tissue infections • “Febrile illness” • Sepsis syndrome
“Front- end” of empiric prescribing High burden of infection admissions Some evidence of poor quality of prescribing National TARGET for antibiotic prescribing in acute medicine and other units Key Issues Identification of infection [education] Severity assessment Use of “investigations” Over treatment and under-treatment Appreciation of “collateral” damage Discussion of unintended consequences Timeliness of antibiotics Why acute medicine ?
Clinical appropriateness and treatment success by severity:SSTI’sMarwick C et al in press
Why acute medicine? • Recognising infection and its severity • Appropriate “empiric” antibiotics • Maintain effectiveness but reduce “collateral damage” • Improve case record documentation • Reduce over diagnosis, over-treatment and under-treatment : UTI, SSTI • Look at use and interpretation of investigations • Engage the “team” in prescribing • Improve timeliness • Look how we can get reliable, sustained improvement
Health, Efficiency & Access to Treatment (HEAT) Targets“30% REDUCTION IN CDADBY MARCH 2011” • Hospital-based empirical prescribing: antibiotic prescriptions are compliant with the local antimicrobial policy and the rationale for treatment is recorded in the clinical case note in >95% of sampled cases • Surgical antibiotic prophylaxis: duration of surgical antibiotic prophylaxis is <24 hours and compliant with local antimicrobial prescribing policy in > 95% of sampled cases • Primary Care empirical prescribing: seasonal variation in quinolone use (summer months vs. winter months) is < 5%, calculated from PRISMS data held by NHS Boards.
Compliance with a combined measure of empirical antimicrobial prescribing in 14 NHS Boards in Scotland (Data poster April 2010)
Impact of restricted policy on CDAD at NWH Vernaz N et al Antibiotic Reduction CDAD Impact
LOCAL AND NATIONAL IMPACT ON CDI P <0.001 P<0.001
Why acute medicine and SAPG collaboration? • “Our desire to move a philosophy of restriction [restricted policy] and judgement [HEAT Target] to a culture of clinical care that is driven by measuring improvement and learning” • “The right antibiotic for the right patient, at the right time, with the right dose, the right route and cause the least harm to the patient and future patients”