Download
1 / 74
760 likes | 1.19k Vues
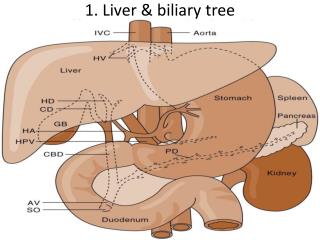
Chapter 18 Liver and Biliary Tract. The liver. Normal adult liver weighs 1400-2600 gm 2.5% of body weight Dual blood supply The portal vein -60-70% The hepatic artery – 30-40% The porta hepatis- hilum – transverse fissure in the inferior surface

E N D
The liver Normal adult liver weighs 1400-2600 gm 2.5% of body weight Dual blood supply The portal vein -60-70% The hepatic artery – 30-40% The porta hepatis- hilum – transverse fissure in the inferior surface Portal tracts- portal veins, hepatic arteries, bile ducts
The liver Hepatic microarchitecture Lobular model 1-2mm hexagonal lobules oriented around the terminal tributaries of the hepatic vein with portal tracts at the periphery Centrilobular Periportal Acinar model Hepatocytes near terminal hepatic veins are apices Penetrating septal venules from the portal vein are the bases Triangle with 3 zones Zone 1 closest to the blood supply Zonation of the parenchyma is important Gradient of activity displayed by many hepatic enzymes Zonal distribution of certain types of hepatic injuries Hepatocytes arranged in sheets Sinusoids between the sheets most richly perfused cells in the body discontinuous endothelial cells space of Disse Kuppler cells Hepatic stellate cells bile canaliculi canals of Hering bile ductulesterminal bile ducts lymphocytes
General Features of Hepatic diseases Major primary diseases of the liver Viral hepatitis Alcoholic liver disease Nonalcoholic fatty liver disease Hepatocellular carcinoma With the rare exception of fulminant hepatic failure, liver disease is insidious, enormous functional reserve Newly diagnosed chronic liver disease -72/100,000 1.1% of al deaths in the US
Laboratory evaluation of liver disease Hepatocyte integrity AST ALT LDH Biliary excretory function bilirubin – total, direct, delta urine bilirubun bile salts AP GGTP 5”-nucleotidase Hepatocyte function Albumin PT Ammonia aminopyrine breath test galactose elimination
Patterns of liver Injury Hepatocyte degeneration and intracellular accumulations Hepatocyte necrosis Inflammation Regeneration Fibrosis Syndromes Hepatic failure Cirrhosis Portal hypertension Disturbances of bilirubin metabolism jaundice, cholestasis
Hepatic failure Acute liver failure associated with encephalopathy within 6 months of diagnosis massive hepatic necrosis drugs or toxins In US 50% acetaminophen 14% other toxins including mushrooms 4% hepatitis A 8% hepatitis B 15% autoimmune and unknown Chronic liver disease – cirrhosis Hepatic dysfunction without overt necrosis tetracyline, acute fatty liver of pregnancy
Hepatic Failure Clinical features jaundice hypoalbuminemia peripheral edema hyperammonemiacerebral dysfunction fetor hepaticus portosystemic shunting impaired estrogen metabolism palmar erythema spider angiomas Males – hypogonadism, gynecomastia Coagulopathy
Hepatic encephalopathy Spectrum of disturbances in consciousness Rigidity, hyper-reflexia, asterixis Disorder of neurotransmission in the CNS and neuromuscular system Minor morphologic changes in the brain Reversible Associated with elevated ammonia levels
Hepatorenal syndrome Appearance of renal failure in patients with severe chronic liver disease 8% per year among patients with cirrhosis and ascites Precipitating stress factor Poor prognosis
Hepatopulmonary syndrome Triad – chronic liver disease, hypoxemia, intrapulmonary vascular dilations Enhanced production of NO by the lung key mediator Respond to O2 Diffusion-perfusion defect
Cirrhosis Chief worldwide causes Alcohol abuse Viral hepatitis NASH ( non-alcoholic steatohepatitis) Three main morphologic characteristics Bridging fibrous septa Parenchymal nodules Disruption of the architecture of the entire liver
Cirrhosis Pathogenesis death of hepatocytes extracellular matrix deposition vascular reorganization Predominant mechanism of fibrosis proliferation of the hepatic stellate cell activation of these cells into highly fibrogenic cells Shunting of blood from the parenchyma Loss of fenestration of the sinusoidal endothelial cells Stimulus for hepatic stellate cell proliferation chronic inflammation cytokine and chemokine production by Kuppler cells, endothelial cells,hepatocytes, and bile dust endothelial cells disruption of the ECM direct stimulation of the stellate cell by toxins Surviving hepatocytes stimulated to regenerate as nodules Result is a fibortic nodular liver delivery of blood to the hepatocytes is compromised ability of hepatocytes to secrete substances into the plasma is compromised Biliary channels are obliterated Clinical features Nonspecific- anorexia, weight loss, weakness, Then signs of hepatic failure Mechanism of death in most progressive liver failure complication related to portal hypertension development of hepatocellular carcinoma
Portal hypertension Prehepatic obstructive thrombosis narrowing of the portal vein massive splenomegaly Intrahepatic cirrhosis Posthepatic severe right-sided heart failure constrictive pericarditis hepatic vein outflow obstruction
Portal hypertension Pathophysiology Increased resistance to flow at the level of the sinusoids Increase in portal venous blood flow resulting from a hyperdynamic circulation arterial vasodilation Role of NO Major clinical consequences ascites formation of portosytemic venous shunts congestive splenomegaly hepatic encephalopathy Pathogenesis of the ascites Sinusoidal hypertension percolation of hepatic lymph into the peritoneal cavity splanchnic vasodilation and hyperdynamic circulation Portosystemic shunts rise in portal system pressure reversed flow from portal to systemic circulation venous bypasses hemorrhoids esophageal varices*** massive hematemesis and death retroperitoneum falciform ligament of the liver (periumbilical and abdominal wall) caput medusae* hallmark of portal hypertension Splenomegaly massive congestion secondary thrombocytopenia or pancytopenia
Jaundice and Cholestasis Common causes of jaundice bilirubin overproduction hepatitis obstruction of the flow of bile Two major functions of bile emulsification of dietary fat in the lumen of the gut through the detergent action of bile salts elimination of bilirubin, excess cholesterol, xenobiotics and other waste products that are not water-soluble enough to be eliminated by the kidney Metabolism of bilirubin uptake from the circulation intracellular storage conjugation with glucoronic acid biliary excretion
Bilirubin and bile formation Bilirubin is the end-product of heme degradation Heme to biliverdin via heme oxygenase Biliverdin to bilirubin via biliverdin reductase Bound to albumin and transported to the liver Uptake by the hepatocytes and conjugated by UDP-glucuronic transferase Excreted into the bile Deconjugated in the bowel by bacteria to urobilinogens and excreted in the feces Enterohepatic circulation Bile acids in bile salts are highly effective detergents for lipids secreted by the hepatocytes into the bile and dietary lipids in the bowel lumen
Pathophysiology of Jaundice Unconjugated bilirubin is virtually insoluble in water at physiologic pH and exists in tight complexes with albumin A very small amount exists as albumin-free anion in plasma – can increase if becomes unbound from albumin by protein-binding drugs or in severe hemolytic disease can diffuse into tissues - kernicterus
Pathophysiology of jaundice Conjugated bilirubin is soluble,non-toxic and only loosely bound to albumin Exess can be excreted in the urine Delta bilirubin is covalently bound to albumin if there is prolonged elevated conjugated hyperbilirubinemia
Pathophysiology of jaundice Jaundice occurs when the equilibrium between bilirubin production and clearance is disturbed by: Unconjugated Excessive extrahepatic production Reduced hepatocyte uptake Impaired conjugation Conjugated Decreased hepatocellular excretion Impaired bile flow
Causes of jaundice Unconjugated Excess production Hemolytic anemias Resorption of blood from internal hemorrhage Ineffective erthropoiesis Reduced hepatic uptake Drug interference with membrane carrier system Some cases of Gilbert syndrome Impaired bilirubin conjugation Physiologic jaundice of the newborn Breast milk jaundice Genetic deficiency of UGT1A1 activity Gilbert syndrome Diffuse hepatocellular disease Conjugated Deficiency of canalicular membrane transporters impaired bile flow
Hereditary Hyperbilirubinemias Unconjugated Crigler-Najjar syndrome Type I Type II Gilbert syndrome Conjugated Dubin-Johnson syndrome Rotor syndrome
Cholestasis Impaired bile formation and flow Accumulation of bile pigment in the hepatic parenchyma - feathery degenerationbile lakes Extra hepatic or intrahepatic obstruction of bile channels Defects in hepatocyte bile secretion Clinical jaundice, pruritus, skin xanthomas, malabsorption, fat-soluble vitamin deficiency elevated AP, GGTP Progressive Familial Intrahepatic Cholestasis PFIC -1,2,3
Infectious disorders Viral hepatitis A,B,C,D,E,G HAV benign, self-limited disease incubation 3-6 weeks ssRNA never causes chronic liver disease sporadic febrile disease Vaccine available
Viral hepatitis HBV Acute hepatitis with recovery nonprogressive chronic hepatitis progressive chronic disease ending in cirrhosis fulminant hepatitis with massive liver necrosis asymptomatic carrier state 10% chronic liver disease partiallly dsDNA Vaccine available incubation 1-4 months highest carrier rate is in perinatally acquired infection HBV genome codes for core protein envelope gycloproteins polymerase HBx HBsAg Anti-HBs HBeAg HBV-DNA DNA polymerase anti –HBc the host immune response is the prime determinant of the outcome of infection
Viral Hepatitis HCV the most common chronic blood-borne infection ssRNA incubation 7-8 weeks 80% chronic liver disease most common cause of chronic liver disease in the US and the most common reason for liver transplant Risk factors IV drug use (54%) multiple sex partners surgery within last 6 months needle stick injury multiple contacts with HCV-infected person employment in medical or dental field unknown (32%) inherently unstable, multiple genotypes and subtypes, quasispecies hampered vaccine efforts elevated titers of anti-HCV IgG occurring after an active infection do not consistently confer effective immunity Characteristic feature of HCV infection is repeated bouts of hepatic damage, the result of reactivation of a preexisting infection or emergence of an endogenous, newly mutated strain 85% acute infection is asymptomatic HCV RNA to assess viral replication
Viral hepatitis HDV Circular defective ssRNA dependent on HBV for its life cycle Acute coinfection with HBV established first Superinfection of chronic carrier Helper-dependent latent infection in liver transplant setting
Viral hepatitis HEV ssRNA incubation 4-5 weeks No chronic liver disease fecal-oral zoonotic high mortality rate in pregnant woman – 20%
Viral hepatitis HGV not hepatotropic bone marrow and spleen no human disease somewhat protective against HIV disease if coinfecting a HIV+ person
Viral hepatitis Clinicopathologic Syndromes Acute asymptomatic hepatitis with recovery ( serologic evidence only) Acute symptomatic hepatitis with recovery ( anicteric or icteric) Chronic hepatitis with or without progression to cirrhosis Fulminant hepatitis with massive to submassive hepatic necrosis Carrier state
Viral hepatitis Acute Ballooning degeneration macrophage aggregates apoptosis bridging necrosis Kuppler cell hypertrophy and hyperplasia portal tract infiltration with inflammatory cells interface hepatitis ductular reaction
Viral hepatitis Chronic smoldering hepatocyte apoptosis lymphoid aggreagtes bile duct reactive changes macrovesicular steatosis interface hepatotis bridging necrosis deposition of fibrous tissue
Other liver infections Toxic shock – Staph.aureus Typhoid fever – Salmonella typhi Syphilis – T.pallidum Ascending cholangitis Parasitic – malaria,schistosomiasis, strpngtloidiasis, cryptosporidosis, leishmaniasis, echinococcosis, liver flukes Abscesses Developing countries – echinococcal and amebic Developed countries – pyogenic portal vein arterial supply ascending from then biliary tract direct invasion from nearby source penetrating injury Fever, RUQ pain, tender hepatomegaly, jaundice
Autoimmune hepatitis Unknown etiology Chronic and progressive Triggers – viral infections, drugs, herbal products Conurrently with other autoimmune disorders Female predominance Clusters of plasma cells in the interface of portal tracts and hepatic lobules Type 1 – ANA, SMA, AAA Anti-SLA/LP Type 2 – ALKM-1, ACL-1 Treatment – immunosuppressives, transplant – can recur in transplanted livers
Drug and Toxin-Induced Liver disease Drug-induced liver injury 10% of adverse drug reactions most common cause of fulminant hepatitis in US Injury from: direct toxicity hepatic conversion of xenobiotic to an active toxin immune mechanisms Predictable(intrinsic) or unpreditable(idiosyncratic) Reye syndrome Exposure to a toxin or therapeutic agent should always be included un the differential diagnosis of liver disease
Alcoholic liver Disease Three forms Hepatic steatosis-reversible if abstention from further alcohol shunting away from catabolism to lipid biosynthesis impairedassembly and secretion of lipoproteins, inreased perioheral catabolism of fat Alcoholic hepatitis-hepatocyte swelling and necrosis, Mallory bodies, neutrophilic reaction, fibrosis acealdehyde Cytochrome P-450 active oxygen species oxidative injury malnutrition and vitamin deficiencies release of bacterial endotoxin from the gut inflammatory response release of endothelins from sinusoidal endothelial cells decrease in sinusoidal perfusion Cirrhosis Pathogenesis Gender, ethnic, genetic, comorbid conditions Steatosis, dysfunction of mitochondrial and cellular membranes, hypoxia, oxidative stress
Metabolic Liver Disease NAFLD Hepatic steatosis Steatosis accompanied by minor, non-specific inflammation NASH Most common cause of chronic liver disease in the US Obesity and metabolic syndrome
Hemachromatosis Excessive accumulation of iron Abnormal regulation of intestinal absorption of dietary iron Micronodular cirrhosis Diabetes mellitus Skin pigmentation AR Slow progression – 5-6th decade Men> women HFE- adult form HJV- juvenile form Deposition of hemosiderin in liver, pancreas,myocardium, oituitary, adrenal, thyroid and parathyroid, joints,skin Cirrhosis Pancreatic fibrosis Clinical – hepatomegaly, abdominal pain,skin pigmentation,diabetes, ardiac dysfunction,arthritis, hypogonadism 200-fold increase risk of hepatocellular carcinoma – treatment for iron overload does not remove the risk Removal of excess iron can reverse the toxic changes if cells are not fatally injured
Neonatal hemochromatosis Not inherited Unknown etiology No treatment Damage begins in utero
Hemosiderosis ( secondary hemochromatosis) Parenteral iron overload Ineffective erythropoiesis withincreased erythroid activity Increased oral intake of iron- Bantu siderosis Congenital atransferrinemia Chronic liver disease
Wilson disease AR Impaired copper excretion into the bile Failure to incorporate copper into ceruloplasmin Toxic levels of copper in brain, liver, eye Kayser-Fleisher rings Clinical- 6-40 years of age Acute or chroni liver disease, neuropsychiatric manifestations, tremor Decrease in serum ceruloplasmin, inrease in liver copper, increased urinary secretion of copper Chelation therapy or zinc-based therapy very sucessful if recognized early
Alpha 1-Antitrypsin deficiency AR Major function of this protein is the inhibition of proteases released from neutrophils Without it pulmonary emphysema and liver disease develop Cutaneous panniculitis, arterial aneurysm, bronchiectasis, Wegener’s granulomatosis Neonatal hepatitis with cholestatic jaundice in 10-20% of newborns with the deficiency
Neonatal Cholestasis 1/2500 live births Prolonged conjugated hyperbilirubinemia Cholangiopathies (primarily biliary atresia) Neonatal hepatitis Major causes Bile duct obstruction neonatal infection toxic metabolic disease miscellaneous idiopathic Imporant to differentiate biliary atresia( needing surgical intervention) Biopsy shows multinucleated giant hepatocytes in neonatal hepatitis
Intrahepatic Biliary Tract disease Secondary Biliary cirrhosis Prolonged obstruction of the biliary tree Gallstones or malignancy or strictures in children biliary atresia CF choledochal cysts pauity of bile ducts (Alagille) proliferation of smaller bile ductules bile lakes feathery degeneration ascending infections – Gram- enteric organisms
Intrahepatic Biliary tract disease Primary Biliary cirrhosis nonsuppurative, inflammatory destruction of medium-sized intrahepatic bile ducts Autoimmune? antimitochondrial antibodies females> males 6:1 fatigue, pruritus, hepatomegaly, hyperpigmentation, eyelid xanthelasmas,arthropathy Small-duct biliary fibrosis and cirrhosis dense accumulation of lymphocytes,macrophages,plasma cells, and occasional eosinophils Extrahepatic manifestations of autoimmunity Sjogren syndrome, systemic sclerosis, thyroiditis, RA, Raynaud’s, membranous GN, celiac disease Treatment with ursodeoxycholic acid – mechanism of action?, remission and prolonged survival in 25-30% 5
Intrahepatic BiliaryTract disease Primary Sclerosing cholangitis Inflammation and obliterative fibrosis of intrahepatic and extrahepatic bile ducts, with dilation of preserved segments Associated with IBD Cholangiocarcinoma
Anomalies of the biliary trees Von Meyenburg Complexes bile duct hamartomas Polycystic liver disease Congenital hepatic fibrosis Caroli Disease All of the above can be associated with polycystic kidney disease Alagille Syndrome (paucity of bile ducts) AD chronic cholestasis, peripheral stenosis of the pulmonary artery, butterfly-like vertebral arch defects, posterior embryotoxon (eye defect) hypertelic facies