Download
1 / 44
590 likes | 1.26k Vues
Cancer and the immune system. BS963 Elena Klenova, e-mail: klenovae@essex.ac.uk. Recommended reading. Immunobiology : the immune system in health and disease / Charles A. Janeway , Paul Travers, Mark Walport and Mark Shlomchik ; 2005, Garland Science Publishing

E N D
Cancer and the immune system BS963 Elena Klenova, e-mail: klenovae@essex.ac.uk
Recommended reading • Immunobiology : the immune system in health and disease /Charles A. Janeway, Paul Travers, Mark Walport and Mark Shlomchik; 2005, Garland Science Publishing • Janeway'simmunobiology 7th ed. / Kenneth Murphy, Paul Travers, Mark Walport ; with contributions by Michael Ehrenstein ... [et al.]; 2009, Garland Science Publishing • The Immune system/Peter Parham, 2005, Garland Science Publishing • Cellular and molecular immunology / Abul K. Abbas, Andrew H. Lichtman, ShivPillai/ 2007, Philadelphia : Saunders Elsevier ( also the 2005 Edition) • Dunn GP, Koebel CM, Schreiber RD: Interferons, immunity and • cancer immunoediting.Nature Reviews Immunology 2006, 6:836-848. • Ichim, C.V. Revisiting immunosurveillance and immunostimulation: Implications for cancer immunotherapy J Transl Med 3, 8 (2005). • Pardoll D. Does the immune system see tumors as foreign or self? Annu. Rev. Immunol. 2003, 21:807-39 • Smyth, M. J. et al. A fresh look at tumorimmunosurveillance and immunotherapy. Nature Immunology 2001, 2: 293 – 299.
Plan of the seminar General Introduction ( Cancer and Immune system). Theories of the role of the immune system in cancer. Cells of the immune system involved in anti-tumour response and basic mechanisms of anti-tumour immunity. Tumours antigens: novel or over-expressed proteins produced by tumours that may be recognized by the immune system. How do tumour cells escape from the immune system? Anti-tumour therapy. Anti-tumour vaccines.
Cancer • Uncontrolled growth produces a tumour ( neoplasm). • Benign - a tumour that is not capable of indefinite growth. It does not kill the host. • Malignant - a tumour that grows indefinitely and often spreads (metastasis). It can kill the host.
Types of Cancer (based on the type of affected tissue) • Carcinoma: Cancer of endo or ectoderm e.g. Skin or epithelial lining of organs. • Sarcomas: Cancer of mesoderm e.g. bone. • Leukemias and Lymphomas: Cancers of hematopoietic cells
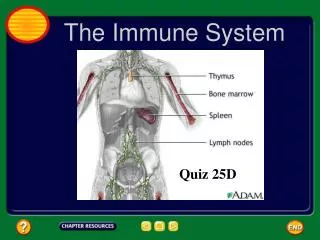
The Immune System Innate (non-specific) immune system (Granulocytes, Macrophages) – immediately available for combat Adaptive (specific) immune system (T – and B-Lymphocytes) – Production of antibody (Ab) or cells specific to combat a particular antigen
Innate and adaptive responses work together Adaptive • Antigen-dependent • Slower (days) • T cells • B cells Innate • Antigen independent • Immediate (hours) • Neutrophils • NK (Natural Killer) cells • Macrophages • Dendritic cells – a link between the innate and adaptive systems! Innate immune responses help form adaptive immune responses, and Adaptive immune responses utilize the machinery of innate immunity for effector function
Evidence for the role of immune system in tumor rejection • Spontaneous regression • Regression of metastases after removal of primary tumor • Regression after chemotherapy • Infiltration of tumors by lymphocytes and macrophages • Lymphocyte proliferation in draining lymph nodes • Higher incidence of cancer after immunosuppression/immunodeficiency (AIDS, neonates, aged, transplant patients)
Tumour rejection antigens are specific for individual tumours
Two distinct theories of the role of the immune system in cancer Immunosurveillance - the tumour-suppressing role of the immune system. Immunostimulation - the tumour-promoting role of the immune system. Tumour and immune system interact: mutual influence!
Immunosurveillance (immune surveillance ) As early as 1909 Paul Ehrlich postulated that cancer occurs spontaneously in vivo and that the immune system is able to both recognize and protect against it . In the late 1950s Lewis Thomas introduced the theory of immunosurveillance, which was subsequently developed by Sir MacFarlane Burnet . The theory states that immunosurveillance is a physiologic function of the immune system. Cancerous cells seen as foreign and thus can be constantly eliminated by immune surveillance. Ichim, C.V. J Transl Med 3, 8 (2005).
Increased incidence of virally-induced tumours in • Immunosuppressed patients • Studies showing increase in de novo malignant • melanoma in organs transplant patients • 25-fold increase in incidence of lung • carcinoma in cardiac transplant patients • Reverse correlations between tumour infiltrating • lymphocytes and tumour survival • Dunn et al. Nature Reviews Immunology 6, 836–848 • (2006) Cancer immunosurveilance: evidence in humans
Cancer immunosurveilance: evidence in mice Dunn et al. Nature Reviews Immunology 6, 836–848 (2006)
Immunostimulation (immune stimulation) The proof of the principle that an inappropriate type of immune response will enhance tumour growth was demonstrated as early as 1907 by Flexner and Jobling, who showed that injection of dead autologoustumour cells enhanced the growth of pre-existing tumours. In 1972, Richmond Prehn formulated the theory of immunostimulation of tumour growth. This theory states that, in contrast to the strong immune response generated by transplantable tumours, a quantitatively mild immune response, such as that generated by spontaneous tumors, is stimulatory to the growth of neoplasia.
How the conflicting roles of the immune response in neoplasia can be explained? • Modern view: The immune system is not a single entity, but a complex system of constituents. The concept of immunosurveillance has been modified and is now considered in three phases: • “Elimination phase” - recognition and destruction of the tumour cells • “Equilibrium phase” – occurs if elimination is not successful. Tumour cells undergo changes in a process called immunoediting. • “Escape phase”- tumour cells evolved enough to grow unimpeded and form a tumour
3. Cells of the immune system involved in anti-tumour response and basic mechanisms of anti-tumour immunity.
The immune system provides one of the body's main defenses against cancer. IFN-g Natural IFN-g When normal cells turn into cancer cells, some of the antigens on their surface change. These new or altered antigens flag immune defenders, including cytotoxic T cells, natural killer cells, and macrophages.
Cells of the immune system involved in tumour response Functions: Phagocytosis Antigen presentation to T cells Phagocytosis of microorganisms and antigen presentation to T cells Kill tumor and virus-infected cells Regulates humoral and cell-mediated immune responses
T-cell classification Classification is based on the Structure & antigen specificity of TCR (T-cell receptor) T cells are divided into two major groups: CD4+ T-helper and CD8+ T-cytotoxic cells. The differentiation of T cells into CD4 vs. CD8 occurs during their development in the thymus. T cells: CD 4 & 8 Accessory Molecules CD4 + helper T cells (TH); further subdivided into type 1 and type 2, also known as Th1 and Th2. The differentiation of Th cells into Th1 and Th2 occurs only after these cells have been activated during an immune response, in the peripheral lymphoid system. - Only recognize antigen bound to MHC class II molecule CD 8 + cytotoxic T cells (TC) Only recognize antigen bound to MHC class I molecules T cells require two signals for activation: 1 -from TCR /MHC-antigen complex & CD4 or CD8/MHC complex 2-from an accessory molecule CD28 When all appropriate signals are received, T-cells clonally expand as a result of IL-2 secretion forming a population of T-cells with the same antigen specificity----further differentiation into memory & effector cells
MHC-Major Histocompatibility Complex: Role of MHC Molecules • Membrane-bound glycoproteins • - Class I and Class II MHC molecules • - MHC genes highly polymorphic-within each species there are many • different forms (alleles) • MHC function as antigen-recognition molecules • - Can bind to a spectrum of antigenic peptides; polymorphism allows • for diversity in antigen recognition • MHC I ---expressed on all nucleated cells • - Present endogenous antigens • CD 8 + (Tc cells) -recognize antigen on MHC I • MHC II ---expressed on Antigen presenting cells (APC) • - Present exogenous antigen • - CD 4 + (Th cells) -recognize antigen on MHC II
Anti-tumour immunity: basic mechanisms Immunology 7th Ed ( D. Male et al)
Antigen – presenting cells (APC) • Dendritic Cells (DC) • DCs are the interface between innate and adaptive immunity • DCs are immature as they circulate waiting to encounter pathogens. At this point, they are highly phagocytic, but not good stimulators of adaptive T cell responses • Once they are activated, they secrete cytokines to initiate inflammation and then they migrate to lymph nodes and mature • As mature DCs they are very efficient APCs for T cell stimulation • Other APCs: macrophages, neutrophils, B-lymphocytes, monocytes.
Anti-tumour immunity: basic mechanisms • Presence of tumour cells • and tumour antigens may • initiate the release of • “danger” signals; cytokines, • heat shock proteins (HSP), • uric acid etc. • • Activation and maturation of dendritic cells, which • present tumour antigens to • CD8 and CD4 cells • Clonal expansion of CD8 and CD4 T cells; migration from the lymph node • • Subsequent T cell mediated destruction of tumour cells Smyth, M. J. et al. Nature Immunology 2, 293 - 299 (2001)
The cellular basis of tumour immunology: CTL - tumor cell interactions
Natural Killer (NK) Cells • First identified by having the ability to lytically kill certain tumor cell lines without prior sensitization • Kill target cell by release of cytotoxic granules containing granzymes and perforin which penetrate target cell membrane and induce programmed cell death • Can mediate Antibody-Dependent Cellular Cytotoxicity (ADCC); (mechanism of immunologic lysis in which cellular targets sensitized by specific antibodies are efficiently and selectively lysed by nonspecific effectors) • Kill virally-infected cells with missing MHC class I • Activated by IFN-a/b or IL-12 (produced rapidly by activated macrophages) • Activated NK cells secrete IFNg, acts on macrophages to increase microbial phagocytosis and killing Fig 8-3
Basic facts about NK cells They get easily activated, do not adapt and kill MHC-negative cells.
4. Tumours antigens: novel or over-expressed proteins produced by tumours that may be recognized by the immune system.
Antigens expressed on tumour cells Major Histocompatability Complex antigens TSTA Tumour-specific transplantation Ag TATA Tumour-associated transplantation Ag TSTA: unique to a tumour Play an important role in tumor rejection. TATA: shared by normal and tumour cells Tumour-associated developmental Ag (TADA) Tumour-associated viral Ag (TAVA)
Tumor-Associated Developmental Antigens • Found on cancer cells and on fetal cells. • Do not trigger anti-tumor immunity. • Used in diagnosis. • Alpha-fetoprotein(AFP) Cancers of liver • Carcinoembryonic Ag (CEA) colorectal cancer
Identification of tumour antigens• Use the immune system as a tool for the identification ofimmunogenic antigens• Gene profiling– genomics or transciptomics• Proteomic approaches– peptidomics, serum profiling• In-silicobioinformatic approaches– probing EST databases
Other Tumor associated antigens Shared tumour antigens: common in different tumours • Cancer-testisantigens MAGE family etc. • Differentiation antigens Melan-A/MART-1, gp100 • Over-expressed proto-oncogenes HER2/neu, WT1 • Some additional antigens MUC-1 (over-expressed) Unique tumour antigens Point mutations: p53, Raf, Bcr/Abl • – viral antigens: HPV, EBV etc.
Malignant cells can be controlled by immunosurveillance NK – Natural Killers CD4, CD8 and gd – types of T-lymphocytes
Ideal tumour antigen: - displays tumour-specific expression - is immunogenic- plays an important functional role in cell survival / differentiation /metastasis etc.
Anti-tumour therapy • Specific • Active Immunization: Vaccination with viral Antigens: e.g. • Hepatitis B virus • Human Papilloma virus (HPV) – success story. • Ab Therapy • Abs specific for oncogene product e.g. Abs against HER2/neu (Herceptin or trastuzumab)
Normal Macro phage Tumor Tumor lysis Activated Macro phage • Nonspecific: • BCG (Bacillus Calmette-Guerin) Mycobacteria used as an adjuvant - melanoma, bladder carcinoma • Irradiated tumour cells ( with or without BCG)
Adoptive immunotherapy– ex vivo manipulation and transfer of effector cells- Antibody-Dependent Cellular Cytotoxicity (ADCC) • Gene therapy Introduce cytokine genes for IL-2, IL-4, IL-12, IFN-g etc into tumor cells to induce immune response. IL-2 T cell tumour IFN-g Macrophages