Download
1 / 17
170 likes | 351 Vues
Trial Vignettes 1-3. Mark Mason Harefield Hospital Royal Brompton and Harefield NHS Trust. MY CONFLICTS OF INTEREST ARE Research grant from Medtronic. EXPORT AMI. 1ry objective:

E N D
Trial Vignettes 1-3 Mark Mason Harefield Hospital Royal Brompton and Harefield NHS Trust
MY CONFLICTS OF INTEREST ARE Research grant from Medtronic
EXPORT AMI • 1ry objective: evaluate flow improvement in pts with AMI within 12 hours of Sx onset undergoing conventional stenting or 1ry aspiration with Export catheter followed by stenting
EXPORT AMI • Primary endpoint: rates of ST resolution >50% (60 minutes post-procedure) and/or Blush grade III; why? • In AMI, TIMI III restored in 94% but normal perfusion in only 28% • Blush 0: no blush • Blush 1: blush but no clearance • Blush 2: blush which clears minimally or not at all in 3 cardiac cycles • Blush 3: blush washes out and clears in 3 cycles
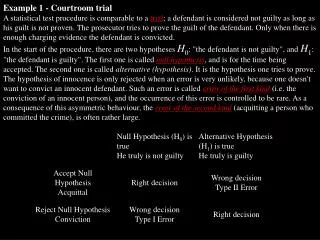
p 1ry endpoint (%) 85 71.9 0.025 No reflow (%) 3.3 10.1 0.04 TIMI frame count 22.82 20.86 0.02 ‘Bailout’ (rescue IIb/IIIa)(%)5.8 14.7 0.02 MACCE @ 30 days(%) 5.8 4.7 0.675 EXPORT AMI
EXPORT AMI • Conclusions • Restoration of TIMI III flow does not necessarily prevent infarction • Use of Export aspiration device appears safe • Routine use of Export device appears associated with improvements in surrogates of microvascular reperfusion (disappointing that there is no attempt to evaluate final infarct size- ?underpowered) • No difference in MACCE at 30 days
HORIZONS AMI • Assessed at 30 days, 6 months and 1-5 years • Primary objectives: • Bivalirudin offers equivalence or reduction in composite of MACE and major bleeding • Bivalirudin offers equivalence or reduction in major bleeding • Includes all-comers inc. LMS and shock
UFH + GP IIb/IIIa Inhibitor N=1802 Bivalirudin Monotherapy N=1800 HORIZONS AMI • 30 day results (stent randomisation still blinded): • F/U available for 1778 UFH arm vs. 1777 Bivalirudin CABG Primary PCI Deferred PCI Medical Rx
HORIZONS AMI Diff = -2.9% [-4.9, -0.8] RR = 0.76 [0.63, 0.92] PNI ≤ 0.0001 Psup = 0.006 Diff = -3.3% [-5.0, -1.6] RR = 0.60 [0.46, 0.77] PNI ≤ 0.0001 Psup ≤ 0.0001 Diff = 0.0% [-1.6, 1.5] RR = 0.99 [0.76, 1.30] Psup = 1.00 1 endpoint 1 endpoint • *Not related to CABG • **MACE = All cause death, reinfarction, ischemic TVR or stroke
30 day Stent Thrombosis UFH + GP IIb/IIIa (N=1553) Bivalirudin (N=1571) P Value ARC definite or probable* 1.9% 2.5% 0.33 - definite 1.4% 2.2% 0.11 - probable 0.5% 0.3% 0.26 - acute (≤24 hrs) 0.3% 1.3% 0.0009 - subacute (>24 hrs – 30d) 1.7% 1.2% 0.30 *Protocol definition of stent thrombosis, CEC adjudicated Overall mortality at 30 days 3.1% UFH vs. 2.1% Bivalirudin, p=0.048
HORIZONS AMI • Conclusions • There appears to be a clear treatment difference at 30 days • This appears to be exclusively due to a reduction in bleeding complications • There does appear to be a lower mortality with bivalirudin at 30 days BUT • There is a significantly higher incidence of acute stent thrombosis
AMIHOT II (!) • AMIHOT I • 269 pts with anterior or large inferior MI, TIMI < 2, undergoing primary or rescue PCI within 24 hours of symptoms • I/C supersaturated O2 post-PCI for 90 minutes • No overall difference in infarct size, ST resolution, improvement in regional wall motion BUT • Anterior infarcts reperfused within 6 hours had reduced infarct size, higher incidence of complete ST resolution and more improvement in regional wall motion
AMIHOT II • Anterior MI reperfused by stenting within 6 hours • TIMI < 2 at presentation • Two primary endpoints: • Efficacy- infarct size (superiority) by SPECT sestamibi at 14 days • Safety- 30 day MACE (non-inferiority) ‘Bayesian hierarchical modelling’ allowed for pooling of data from AMIHOT I and II (!)
AMIHOT II • No difference in primary endpoints in AMIHOT II • No difference in proportion with ‘0%’ infarcts • HOWEVER………
AMIHOT II • When AMIHOT I and II pooled: • Infarct size reduced (p=0.023) • Higher proportion of ‘0%’ LV infarcts (18.3% SSO2 vs. 10.3%, p=0.03) • No difference in MACE • 4.7% all pts/3.8% AMIHOT II + ant MI < 6hrs AMIHOT I Vs. 5.9%/5.5% respectively, p= 0.57/0.48
AMIHOT II • Observations: • AMIHOT II was a negative study • Questionable clinical validity of pooling data in this way • Study groups chosen at opposite extremes- • < 6 hours includes pts who would do well anyway • Up to 24 hours will include pts who will not do well regardless • SPECT data might be more useful if ‘acute’ and ‘convalescent’ scan performed • Conclusions: • This evidence does not suggest any clinically useful myocardial salvage