Download
1 / 34
580 likes | 2.92k Vues
Inserm Unit 845 , Research Center Growth & Signaling, Faculty of Medicine Necker, Paris. Dept Endocrinology & Reprod uctive Medicine, Hospital Pitié Salpetrière, Paris. Premature Ovarian Failure. Santiago, October 5th, 2007 Pr Philippe Touraine philippe.touraine@psl.aphp.fr.

E N D
Inserm Unit 845, Research Center Growth & Signaling, Faculty of Medicine Necker, Paris Dept Endocrinology & Reproductive Medicine, Hospital Pitié Salpetrière, Paris Premature Ovarian Failure Santiago, October 5th, 2007 Pr Philippe Touraine philippe.touraine@psl.aphp.fr
5 th Week of embryogenesis Endodermal stem cells Genital crest Ovogonia Oogonia Mitosis Meiosis Atresia Maximal at 20thWeek 28th Week Primary Oocytes 8th week : 600 000 oogonia
6-7 Million germ cells at 20th Week • 2/3 are oocytes in meiosis • 1/3 are oogonia Atresia • < 20 % germ cells at birth la naissance • 300 000 at puberty • 400-500 follicles during genital life
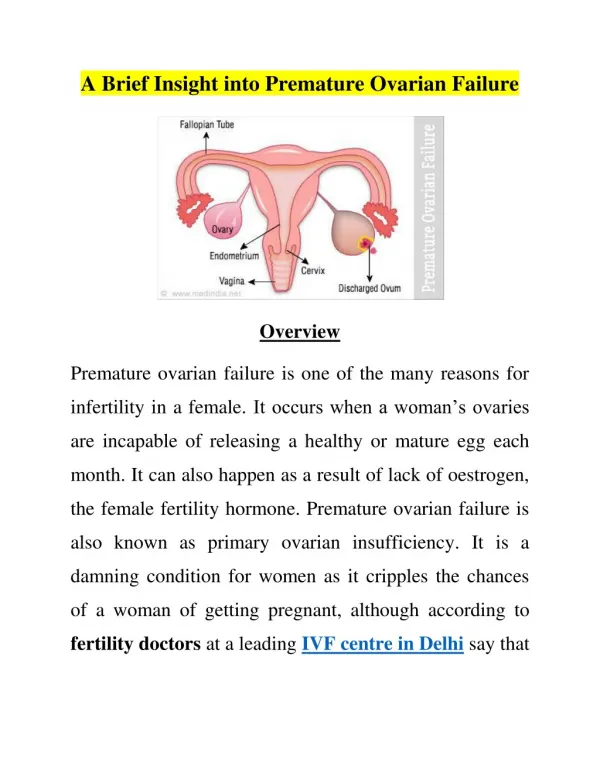
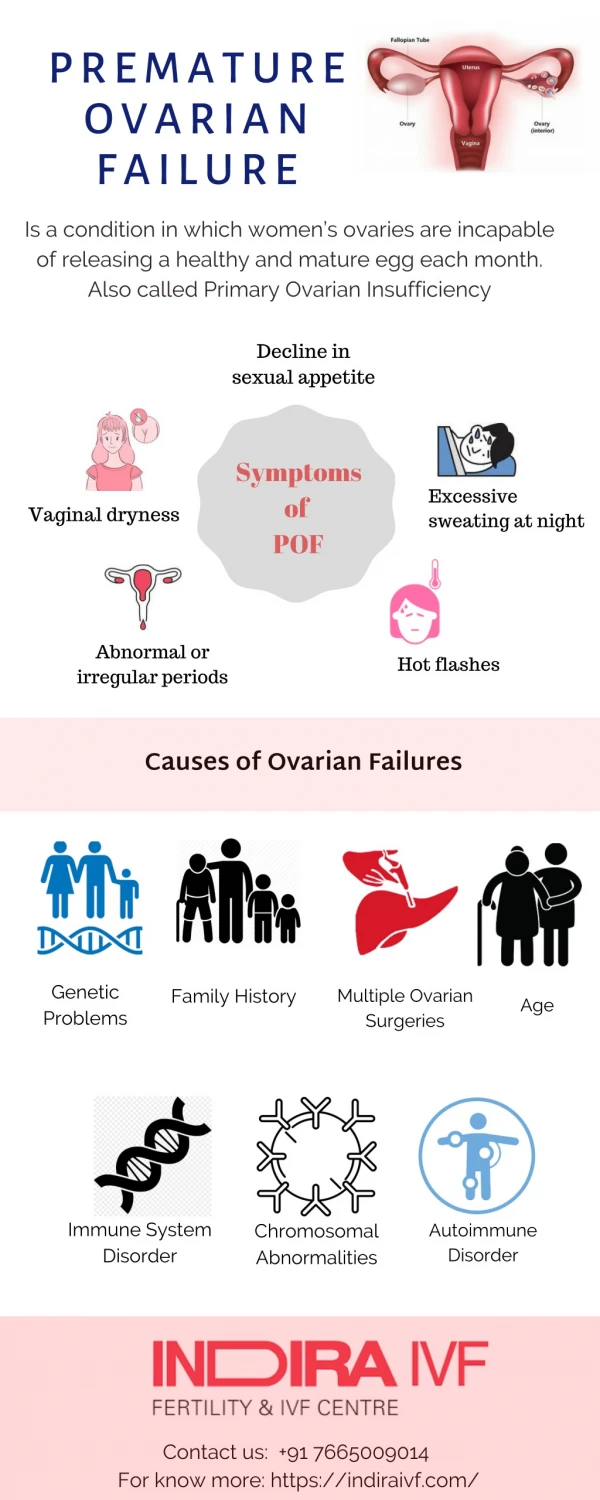
Premature Ovarian Failure (POF) • WHO : Permanent Cessation of menstruations secondary to loss of follicular activity • Characterized by : • Women < 40 yrs • Amenorrhea > 4 months • Hypergonadotrophic Hypogonadism (FSH > 30 UI/L) Anasti JN, Fertil. Steril., 1998, 70 : 1-5. • Incidence : # 1% Coulam CB et al., Obstet. Gynecol., 1986, 67 : 604-6
Autoimmunity FSHR anomalies Cx37, GDF9, BMP-15 Enzyme deficiencies Follicular Depletion Chemotherapy X chromosome anomalies Autoimmunity Follicular Dysfunction Accelerated atresia Premature Ovarian Failure 1% of 40-year-old-women Etiology most often remains unknown
Follicular Depletion Chemotherapy X chromosome anomalies Autoimmunity Accelerated atresia Premature Ovarian Failure
% cases with POF Total of cases with POF Primary amenoorhea Secondary amenorrhea Schlessinger et al., Am J Med Genet, 2002
POF - FMR1 • 20% premutated and 14% grey zone develop POF (Bretherick, 2005) • 13-21% familial forms POF are premutated • 3-7% sporadic POF are premutated (Shermann, 2000) • Prevalence: 0.4% women with normal fertility
Drugs Normal Cycles Normal cycles Oligomenorrhea Amenorrhea POF and chemotherapy Radiotherapy : 6 Gy on ovaries : non reversible POF
Autoimmunity FSHR anomalies Cx37, GDF9, BMP-15 Enzyme deficiencies Follicular Dysfunction Premature Ovarian Failure
Genetics of POF • Is there any argument for a genetic compound • Genes and physiological menopause • Correlation between age of menopause in mother and girls De Bruin, Hum Reprod 2001 • Cohort of twins: POF described in up to 63% Snieder, J Clin Endocrinol Metab 1998 Gosden R, Hum Reprod, 2007 • Familial cases in 15 to 20%
Ovulation Blocade of follicular maturation Antral Secondary Primary Primordial Atresia Hsueh, Endocrine Review, 2000
Ala189 Val NH2 COOH FSH receptor gene mutation in the Finnish population • 22 patients with primary amenorrhea • Pubertal development variable • Hypoplasic ovaries at histological examination • Presence of primordial and primary follicles
Setting up a POF Network • Phenotyping of the patients (specificities of subgroups) • Constitution of a DNA Bank • Identification of new mutations of genes involved in folliculogenesis • Constitution of an ovarian tissue bank • Immunohistochemistry / steroidogenesis • Ovarian transcriptome • Prospective follow-up of population
Clinical Phenotype Biological Phenotype Morphological Phenotype Questionnaire Karyotype Hormonal evaluation Ultrasonography Laparoscopy - Histology Current Evaluation
351 patients • 50 excluded • 40 yrs • FSH<30 mUI/l • Secondary POF • Karyotype “Turner-like” 74 patients < 18 yrs (25%) 301 patients 8 karyotypic anomalies 293 46,XX idiopathic Bachelot et al., 2007, submitted
20 18 16 14 12 Number of Patients 10 8 6 4 2 0 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 Age at diagnosis (yrs) Mean age: 26.5 ± 7.8 Bachelot et al., 2007, submitted
250 200 150 Number of Patients Puberty 100 absence partial normal 50 0 Primary amenorrhea Secondary amenorrhea Bachelot et al., 2007, submitted
Clinical Phenotype • 41 patients with a history of familial POF • 13.6% des POF • 59 patients with autoimmunity biomarkers • 19.6 % of POF • 37 with thyroid disorders • Diabetes, juvenile arthritis, vitiligo,…. • 6 patients with antiovarian antibodies (IFI) • 41 patients with fluctuating POF • 5 pregnancies; 3 births
134 woman have detectable E2 levels and 58 inhibin B • AMH detectable in 105 patients Bachelot et al., 2007, submitted
Bone Mineral Density • Available for 151 patients • Mean age 28.7 yrs (15-42) • Definition WHO • 66 patients (42%) BMD normal • 63 patients osteopenia (42%), 14 at neck and 25 at lumbar • 22 patients osteoporosis (15%), 7 at neck and 20 at lumbar
100µm 100µm Two Different Patterns N = 75 N= 29 Bachelot et al., 2007, submitted
Ovarian Histology 70 60 Follicular Histology 50 antrum Early antral 40 secondary primary primordial 30 Absence of foll 20 10 0 Primary 25% Secondary 70% Bachelot et al., 2007, submitted Amenorrhea
Foll - Foll - 40 Foll + 35 Ultrasonogaphy 30 Foll + 25 20 15 10 5 Histo - Histo + Massin et al., 2004
Pro272Leu Thr Asp224 Val Ile191 Leu Ile160 Thr Ala189 Val NH2 Leu601 Val Pro519 Thr Arg573 Cys Ala419 Thr COOH FSH Receptor gene mutations Patient 1 Patient 2 Patient 3 Beau et al. JCI, 1998Touraine et al., Mol Endocrinol, 1999Meduri et al., JCEM, 2003
Etiology actually possible in 30 patients (10%) • 8 with karyotype anomalies • 5 with FMR1 premutation • 16 anomalies of genes involved in POF • 2 APS type 2, 1 with multiple AI diseases
What to do in our current practice? Clinical evaluation: Height Familial POF syndrome, Syndromic defects, Autoimmunity Karyotype Hormonal evaluation: FSH-E2; Androgens AMH, Inhibine B Ultrasonography: Surface, Presence of Follicles Evaluation of BMD DNA analysis: XFra FSHR analysis in patients with presence of follicles at ultrasonography Hormonal substitution Treatment of infertility Bachelot et al., 2007, submitted
What to say? • Information +++ • Psychological help • HRT • Explanation about pregnancy plans (oocyte donation…) • Discussion about “ovaries to be frozen”
Around POF Diagnosis Gross et al., Fertil Steril, 2005
Radiology C Matuchansky C Balleyguier Hormonal Biochemistry K Laborde Cytogenetics Surgery F Lecuru B Paniel Pathology Cochin CHIC HEGP G Meduri Genetics M Misrahi, Bicêtre M Fellous, Cochin C Cotinot, INRA D Castrillon, Dallas, TX L.Messiaen, Gant, Belgium Department of Endocrinology and Reproductive Medicine Necker Hospital Pr F. Kuttenn Nathalie Massin Anne Bachelot Yvette Le Rouzic Philippe Touraine National and International Collaboration
Team « Centre Maladies rares de la croissance » philippe.touraine@psl.aphp.fr Beau et al. J. Clin Invest, 1998;Touraine et al., Mol Endocrinol, 1999;Meduri et al., JCE&M, 2003; Massin et al., Hum Reprod, 2004; Bachelot et al., JCE&M, 2005; Massin et al., Horm Res, 2006 Meduri et al., Hum Reprod, 2006; Laissue et al., Eur J Endocrinol, 2006