Download
1 / 63
670 likes | 981 Vues
Antimicrobial Drugs. Antimicrobial Drugs. Chemicals used to treat microbial infections Before antimicrobials, large number of people died from common illnesses Now many illnesses easily treated with antimicrobials However, many antimicrobial drugs are becoming less useful.

E N D
Antimicrobial Drugs • Chemicals used to treat microbial infections • Before antimicrobials, large number of people died from common illnesses • Now many illnesses easily treated with antimicrobials • However, many antimicrobial drugs are becoming less useful
Antimicrobial Drugs • Chemotherapeutic agent= • Antimicrobial drug= • Different types of antimicrobial drugs: • Antibacterial drugs • Antifungal drugs • Antiprotozoan drugs • Antihelminthic drugs
Features of Antimicrobial Drugs • Most modern antibiotics come from species of microorganisms that live in the soil • To commercially produce antibiotic: • Select strain and grow in broth • When maximum antibiotic concentration reached, extract from medium • Purify • Chemical alter to make it more stable
Features of Antimicrobial Drugs:Selective Toxicity • Cause greater harm to microorganisms than to host • Chemotherapeutic index: lowest dose toxic to patient divided by dose typically used for therapy
Features of Antimicrobial Drugs: Antimicrobial Action • Bacteriostatic: inhibit growth of microorganisms • Bactericidal: Kill microorganisms
Features of Antimicrobial Drugs:Spectrum of Activity • Antimicrobial medications vary with respect to the range of microorganisms they kill or inhibit • Some kill only limited range : Narrow-spectrum antimicrobial • While others kill wide range of microorganisms: Broad-spectrum antimicrobial
Features of Antimicrobial Drugs:Effects of Combining Drugs • Combinations are sometimes used to fight infections • Synergistic: action of one drug enhances the activity of another or vice versa. • Antagonistic: activity of one drug interferes with the action of another.
Features of Antimicrobial Drugs:Adverse Effects • Allergic Reactions: some people develop hypersensitivities to antimicrobials • Toxic Effects: some antimicrobials toxic at high concentrations or cause adverse effects • Suppression of normal flora: when normal flora killed, other pathogens may be able to grow to high numbers
Features of Antimicrobial Drugs:Resistance to Antimicrobials • Some microorganisms inherently resistant to effects of a particular drug • Other previously sensitive microorganisms can develop resistance through spontaneous mutations or acquisition of new genes (more later).
So, The Criteria of the Ideal Antibiotic: • Selectively toxic to microbe but nontoxic to host. • Soluble in body- tissue distribution – BBB. • Remains in body long enough to be effective - resists excretion and breakdown. • Shelf life. • Does not lead to resistance. • Cost not excessive. • Hypoallergenic. • Microbiocidal rather than microbiostatic. • Concerns suppression of normal flora - antibiotic associated colitis with Clostridium difficule and it’s toxins or Candida albicans.
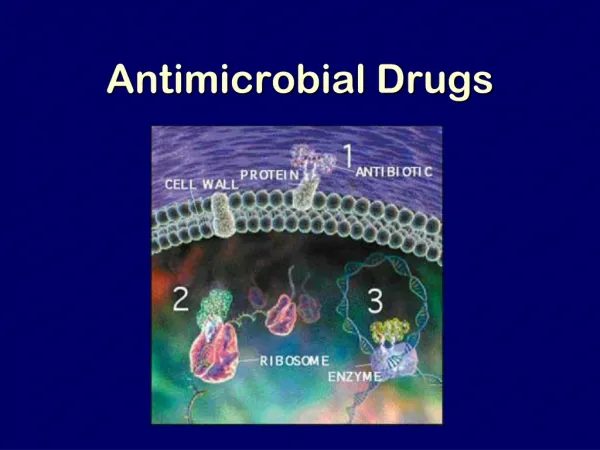
Mechanisms of action of Antibacterial Drugs • Inhibit cell wall synthesis • Inhibit protein synthesis • Inhibit nucleic acid synthesis • Injury to plasma membrane • Inhibit synthesis of essential metabolites
Inhibition of Cell Wall Synthesis:b-Lactam Drugs • Irreversibly inhibit enzymes involved in the final steps of cell wall synthesis • These enzymes mediate formation of peptide bridges between adjacent stands of peptidoglycan • b-lactam ring similar in structure to normal substrate of enzyme • Drug binds to enzyme, competitively inhibit enzymatic activity
b-Lactam Drugs • Some bacteria produce b-lactamase- enzyme that breaks the critical b-lactam ring • b-lactam drugs include: penicillins and cephalosporins
Penicillins (Benzylpenicillin) • Acid-labile. • Gram+ bacteria. • So, take phenoxymethylpenicillin. • Large Vd, but penetration into brain: poor, except when the meninges are inflammed. • Broad spectrum penicillins: amoxicillin and ampicillin are more hydrophillic and therefore, are active against gram- bacteria.
Penicillins (Benzylpenicillin) Penicillinase-resistant penicillins – Flucloxacillin Indicated in infections caused by penicillinase-producing pen-resistant staphlococci. Has an isoxazolyl group at R1 sterically hinders access of the enzyme to the β-lactam ring. Less effective than benzylpen. So, should be used only for pen-resistant infections. Well-absorbed orally, but in severe infections, should be i.v. and not alone. Staphlococci aureas-resistant strains to flucloxicillin and MRSA (methicillin-resistant Staph aureas) – increasing problem.
Broad-Spectrum Penicillins • Ampicillin and amoxicillin – very active against non-β-lactamase-producing gram+ bacteria. • Because they diffuse readily into Gram- bacteria, also very active against many strains of E. coli, H. influenzae, and Salmonella typhimurium. • Orally, amoxicillin is better because absorption is better. • Ineffective against penicillinase-producing bacteria (e.g., S. aureus, 50% of E. coli strains, and up to 15 % of H. influenzae strains. • Many baterial β-lactamases are inhibited by clavulaic acid ± amoxicillin (co-amoxiclav) antibiotic is effective against penicillinase-producing organisms. • Co-amoxiclav indicated in resp and UT infections, which are confirmed to be resistant to amoxicillin.
Cephalosporins • Used for treatment of meningitis, pneumonia, and septicemia. • Same mech and p’col as that of pens. • May allergic rxn and cross-reactivity to pen. • Similar to pens in broad-spectrum antibacterial activity. Cedadroxil (for UTI) in case of antibact resist. Cefuroxime (prophylactic in surgery) – Resistant to inactivation by β-lactamases and used in severe infections (others ineffective). Ceftazidine – wide range of activity against gram- including Pseudomonas aeruginosa), but is less active than cefurozime against gram+ bact (S aureus). Used in meningitis (CNS-accessible) caused by gram- bacteria.
Vancomycin • Not well absorbed orally. • Inhibits peptidoglycan formation. • Active against most gram+ organisms. • I.v. treatment for septicemia or endocarditis caused by MRSA. • Used for pseudomembranous colitis (superinfection of the bowel by Clostridium difficile – produces a toxin that damages the colon mucosa)
Antibacterial Drugs that Inhibit Cell Wall Synthesis
Antibacterial Medications that Inhibit Protein Synthesis • Target ribosomes of bacteria • Aminoglycosides: bind to 30S subunit causing it to distort and malfunction; blocks initiation of translation • Tetracyclines: bind to 30S subunit blocking attachment of tRNA. • Macrolides: bind 50S subunit and prevents protein synthesis from continuing.
Aminoglycosides • Against many gram- and some gram+. • Narrow TI – very potentially toxic. • Most important adverse side-effect: VIIIth cranial n. (ototoxicity) and kidney damage. • Resistance – several mechs: inactivation of the drug by acetylation, phos, or adenylation, Δ envellope to prevent drug access, and Δ the binding site of the 30S subunit (streptomycin only).
Aminoglycosides • Gentamicin – used for acute, life-thretening gram- infections. Has synergism with pen and van and combo. • Amikacin – used for bact that are gent-resistant. • Netilmicin – less toxic than gentamicin. • Neomycin – too toxic for parenteral use. Used for topically for skin infections and orally for sterilizing bowel before surgery. • Streptomycin – active against Mycobacterium tuberculosis. But bec of its ototoxicity, rifampicin replaces. • Rifampicin – resistance develops quickly alone; so, with TB, combine with isoniazid, ethambutol, and pyrazinamide for the 1st 2 mos of treatment, followed by another 4 mos with rifampicin and isoniazid.
Macrolides • Very safe drugs. • Ususally given orally. • Erythromycin and clarithomycin • Effective against gram- bact and can be used as an alt to pen-sensitive patients, esp in infections caused by streptococci, staphylococci, pneumococci, and clostridia. • Don’t cross the BBB – ineffective against meningitis. • Resistance- occurs bec of plasmid-controlled Δ of their receptor on the 50S subunit. • Erythromycin – in high doses, may cause nausea and vomiting (less so with clarithromycin and azithromycin). • Azithromycin – very long t1/2 (~40-60 hr) and a single dose is as effective in treating chlamydial non-specific urethritis as tretracycline admin over 7 days,
Tetracyclines • Broad-spectrum. • Penetrate microorganisms well. • Sensitive organisms accumulate it through partly passive diffusion and partly through active transport. • Resistant organisms develop an efflux pump and do not accumulate the drug. • Genes for tet-resistance transmitted by plasmids. • Closely assoc with those for other drugs to which the organisms will also be resistant (e.g., sulphonamides, aminoglycosides, chloramphenicol). • Tets bind to Ca in growing bones and teeth can discolor teeth. So, should be avoided in children < 8 yrs old.
Chloramphenicol • Broad-spectrum. • Serious side-effects: bone marrow aplasia, suppression of RBCs, WBCs, encephalopathy, optic neuritis. • So, periodic blood counts required, esp in high doses. • Large Vd, including CNS. • Inhibits the actions of other drugs and may incr the actions of phenytoin, sulphonlureas, and warfarin. • Neonates cannot met the drug rapidly accum ‘grey baby’ syndrome (pallor, abdominal distension, vomiting, and collapse).
Antibacterial Drugs that Inhibit Protein Synthesis
Antibacterial Medications that Inhibit Nucleic Acid Synthesis • Target enzymes required for nucleic acid synthesis • Fluoroquinolones: inhibit enzymes that maintain the supercoiling of closed circular DNA • Rifamycins: block prokaryotic DNA-dependent RNA polymerase from initiating transcription
Sulphonamides • Sulfadiazine well-absorbed orally. Used to treat UTIs. • But many strains of E. coli are resistant. • So, use less toxic drugs instead. • Adverse effects: allergic rxns, skin rashes, fever. • Trimethoprin – used for UTIs and Resp TIs • Co-trimoxazole (trimethoprin + sulfamethoxazole) – used mostly for pneumonia, neocarditis, and toxoplasmosis.
Sulfonamides (Sulfa drugs) Inhibit folic acid synthesis Broad spectrum Antibacterials – Competitive Inhibitors Figure 5.7
Quinolones (GABA antagonists) • Inhibit DNA gyrase. • Nalidixic acid – used only for UTIs. • Ciprofloxin (6-fluoro substituent) that greatly enhances its effectiveness against both gram- and gram+ bacteria. Well-absorbed both orally and i.v. Eliminated largely unchanged by the kidneys. Side-effects (headache, vomiting, nausea) are rare; but convulsions may occur.
5-Nitroimidazoles • Wide-spectrum • Metronidazole – against anaerobic bacteria and protozoan infections. • Tinidazole – longer duration of action. • Diffuses into the organism where the nitro group is reduced chemically reactive intermediates are formed that inhibit DNA synthesis and/or damage DNA.
Antibacterial medications that Injure Plasma Membrane • Polymyxin B: binds to membrane of G- bacteria and alters permeability • This leads to leakage of cellular contents and cell death • These drugs also bind to eukaryotic cells to some extent, which limits their use to topical applications
Antibacterial Drugs that Inhibit Synthesis of Essential Metabolites • Competitive inhibition by substance that resembles normal substrate of enzyme • Sulfa drugs
Antiviral Drugs • Very few antiviral drugs approved for use in US • Effective against a very limited group of diseases • Targets for antiviral drugs are various points of viral reproduction
Drugs that Prevent the Virus from Entering or Leaving the Host Cells • Amantadine – interferes with replication of influenza A by inhibiting the transmembrane M2 protein that is essential for uncoating the virus. - Has a narrow spectrum; so, flu vaccine is usually preferable. • Zanamivir – inhibits both influenza A and B neuraminadase. Decr duration of symptoms if given within 48 hr of the onset of symptoms. Prophylactic in healthy adults. • Immunoglobulins – Human Ig contains specific Abs against superficial Ags of viruses can interfere with their entry into host cells. Protection against hepA, measles, and rubellla (German measles).
Drugs that Inhibit Nucleic Acid SynthesisNucleoside and Nucleotide Analogs • Acyclovir- used to treat genital herpes • Cidofovir- used for treatment of cytomegaloviral infections of the eye • Lamivudine- used to treat Hepatitis B
Acyclovir • HSV and VZV contain a thymidine kinase (TK) that acyclovir to a monophosphate phosphorylated by host cell enzymes to acycloguanosine triphosphate, which inhibits viral DNA pol and viral DNA synthesis. • Selectively toxic (TK of uninfected host cells activates only a little of the drug). • Viral enzymes have a much higher affinity than the host enzymes for the drug. • Effective against HSV, but does not eradicate them. • Need high doses to treat shingles.
Ganciclovir • Quite toxic (neutropenia) –so, given only for severe CMV infections in immunosuppressed patients. • CMV is resistant to acyclovir because it does not code for TK.
Antiretrovirals • Currently implies a drug used to treat HIV • Tenofovir- nucleotide reverse transcriptase inhibitor • Zidovudine- nucleoside analog – inhibits RT of HIV and is only used orally for AIDS. - Activated by triple phosphorylation and then binds RT (with100X affinity than for cellular DNA pols). - Incorporated into the DNA chain, but lacks a 3’OH; so another nucleoside cannot form a 3’-5’-phosphodiester bond DNA chain elongation is terminated. -Severe adverse effects: anemia, neutropenia, myalgia, nausea, and headaches. • Stavudine, didanosine, zalcitabine – among other NRTIs. • Nevirapine, efavirenz – Non nucleoside RTIs - denature RT.
Life Cycle of HIV