Download
1 / 77
810 likes | 1.28k Vues
Oxygen Needs Interference with O2 Transport. Case Study. Oxygen Needs Interference with O2 Transport. Coronary Artery Disease Complications Dysrhythmias Pulmonary Embolism Hypertension Complication Congestive Heart Failure Peripheral Vascular / Arterial Disease.

E N D
Oxygen NeedsInterference with O2 Transport
Oxygen NeedsInterference with O2 Transport Coronary Artery Disease • Complications • Dysrhythmias • Pulmonary Embolism • Hypertension • Complication • Congestive Heart Failure • Peripheral Vascular / Arterial Disease
Oxygen NeedsInterference with O2 Transport • Care of Patients with: • Coronary Artery Disease • Risk Factors • Myocardial Infarction • Alterations in: • Rate & Rhythm (Cardiac Conduction) • Effect on Cardiac Output
Content Approach • Anatomy & Physiology Review • Demographics/occurrence • Pathophysiology • Clinical Manifestation • Medical / Surgical Management • Nursing Process (APIE) • Assessment - Nursing Actions - Education
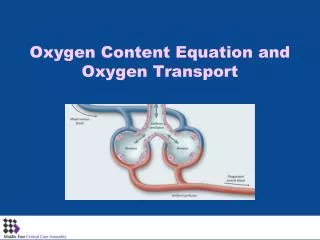
Anatomy & Physiology • Right Heart • Left Heart • Systole • Valve Closure: • Diastole • Valve Closure:
Cardiac Cycle • Passive Filling – preload • Atrial contraction – Aortic & Pulmonic semilunar valves close – S2 • Isovolumetric ventricular contraction – all valves closed • Ejection – ventricular systole – Mitral & Tricuspid valves close – S1 - afterload • Isovolumetric ventricular relaxation – all valves closed
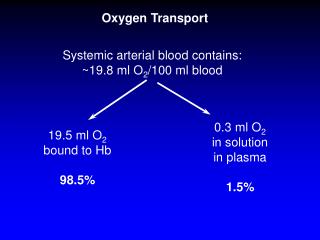
Physiology: Oxygen Supply to the Cardiac Muscle during the Cardiac Cycle • Coronary artery oxygen deficit • during ventricular contraction & ejection (systole) • Coronary artery filling • during ventricular filling (diastole) What is the impact of heart rate on coronary artery filling?
Oxygen Supply to the Cardiac Muscle during the Cardiac Cycle • The actual time available for diastole shortens significantly as the heart rate increase % of a Minute Heart Rate 70% 60 50% 120 33% 188 • Results: Less time for ventricular filling & coronary artery filling + as HR increases, increased oxygen is needed each minute to eject the same volume of blood. Stroke volume: volume ejected in one heart beat Cardiac Output: volume ejected in one minute Cardiac Output = Stroke Volume x Heart Rate
Factors Determining Myocardial Oxygen Needs • Decreased Oxygen Supply: • Noncardiac: Anemia, hypoxemia, pneumonia, asthma, COPD, low blood volume • Cardiac: Arrhythmias/dysrhythmias, congestive heart failure (CHF), coronary artery spasm, coronary artery thrombosis, valve disorders • Increased Oxygen Demand or Consumption: • Noncardiac: anxiety, cocaine use, hypertension, hyperthermia, hyperthyroidism, physical exertion • Cardiac: aortic stenosis, arrhythmias, cardiomyopathy, hypertension, tachycardia
Comparison of death by CV Disease and Breast Cancer – by Women’s Age
Coronary Artery Disease (CAD) Pathophysiology • ASHD, IHD, CVHD = CAD • AHA • 1.1 mil Americans will have an MI in 2003 • 460,000 will die • About half of those deaths occur within 1 hour of the start of symptoms and before the person reaches the hospital. • Major cause: Atherosclerosis—focal deposit of cholesterol & lipids
CAD – Risk Factors • Unmodifiable: Age, Gender, Ethnicity, Genetic predisposition/family history • Modifiable Major: Dyslipidemia--Elevated serum lipids*, hypertension*, cigarette smoking, obesity—visceral/central obesity • Modifiable Contributing: Diabetes Mellitus*, stressful lifestyle * may have genetic predisposition
CAD – Risk Factors • Metabolic Syndrome: • Insulin Resistance • Hyperglycemia >110mg/dL • Hypertension - > 130/85 • Increased triglycerides >110mg/dL • Decrease HDL <40 men; < 50 women • Central Obesity • men: waist > 40” women: waist > 35”
Risk Factors One of the Major Modifiable Physical Inactivity
Types of Plasma Lipoproteins • HDL – • Contain more protein and less lipid • Carry lipids away from arteries to liver for metabolism • This process prevents lipid accumulation within arterial walls • Higher levels are desirable • LDL – • Contain more lipids than any other lipoproteins • Affinity for arterial walls • Increased levels correlate closely with an increased incidence of atherosclerosis • Lower levels are desirable • VLDL • Contain of triglycerides • Correlation with heart disease is uncertain
Atherosclerosis • Elevated serum lipids • Cholesterol > 200mg/dl • Triglyceride > 200mg/dl • HDL • < 35 mg/dl – major risk • 45-59 mg/dl – average risk • > 60 mg/dl – negative risk • LDL • < 130 – desirable • 130 – 159 mg/dl – borderline risk • > 160 mg/dl – high risk
Drug Therapy for Dyslipidemia • Bile Acid Sequestrants (Questran) - Binds with bile salts • Niacin - Inhibits synthesis of VLDL & LDL • Fibric Acid Derivatives (Atromid)– Decrease VLDL • HMG CoA Reductase Inhibitors (Statins - Lipitor, Pravachol, Zocor) – Block synthesis of cholesterol • Cholesterol Absorption Inhibitor (Zetia)– Inhibits intestinal absorption of cholesterol
Natural Lipid Lowering Agents • Niacin - < LDL levels • Omega-3 fatty acids – fish/flaxseed oil - <Triglycerides & > HDL levels • Milk thistle – Silymarin - > HDL levels • Fiber - < Cholesterol • Phytosterols - < Cholesterol • Soy - < Cholesterol absorption from GI tract • CoEnzyme Q10 – HMG CoA reductase inhibitors – natural statins
Clinical ManifestationsAngina – Chest Pain • Stable Angina Pectoris – intermittent, same pattern of onset, duration, intensity of symptoms - 3-5 mins. • Silent Ischemia – 80% of patients with ischemia are asymptomatic • Prinzmetal’s Angina – variant – not precipitated by physical activity – may be due to spasm • Nocturnal Angina – occurs at night but not necessarily during sleep or in recumbent position • Angina Decubitis – recumbent position – relieved by standing • Unstable Angina – Unpredictable or may evolve from stable angina – increasing frequency, duration, intensity
CAD Clinical Manifestation – Diagnostics • History & Physical Examination • EKG / Echocardiogram / Stress Echocardiogram • Thallium Stress Test (perfusion scanning) cold spots where tissue is inadequately perfused cardiac tissue • CAT scan- calcium score/CT coronary angiogram • MUGA (Multiple gated radioisotope scan) – left ventricular function • MRI of the heart • PET (Positron emission computed tomography) – evaluate coronary artery patency
CAD - Clinical ManifestationInvasive Diagnostics • Cardiac Catheterization • Right sided: • Catheter through the femoral vein through the vena cava into right atrium and right ventricle – pulmonary artery – wedge pressure • Left sided: • Catheter through the femoral artery through the aorta into the left atrium and left ventricle / openings of the coronary arteries • Coronary arteriography: Injected dye with video & x-rays
CAD - Clinical ManifestationInvasive Diagnostics • Cardiac Catheterization • Potential Complications • Catheter looping/breaking, dysrhythmias, allergic reaction to contrast medium, arterial thrombosis, myocardial infarction, hemorrhage, infection. • Patient Preparation • Informed consent; allergies – shellfish/iodine; NPO x 6 hrs; explanation “flushed/tingling”; supine – absolutely still • Postprocedure Care
Cardiac CatheterizationPost Procedure Care • Assess: • VS q15 mins. x 2 hrs; q30 min x 2 hrs • Monitor cardiac rate and rhythm • Check site for bleeding • Extremity: Peripheral pulse check, temperature, color, sensation, mobility • Assess for chest pain, dizziness, dyspnea • Nursing Action: • Straight at groin x 24 hours; pressure at site x 30 mins. • Maintain IV KVO for 2 hrs; IV capped x 2 hrs; then d/c • Encourage oral fluids • Patient/Family Education: • Rationale for all nursing actions • No squatting, sitting, lifting for 24 – 48 hours++ • Report bleeding, swelling, discoloration, drainage • Change dressing after 24 hours – small dressing to bandaid
Clinical Manifestation Myocardial Infarction Lab Diagnostics • Cardiac Protein – Troponin T • More sensitive than CK • Elevates 3 hr – peak 24-48 hrs; normal 5-14 days • Cardiac Enzyme – Creatine kinase (CK-MB) • Released when cardiac cells die • Elevates 3 hrs – peak 12-24 hrs; normal 2-3 days • Cardiac Marker - Myoglobin • First to elevate • Lacks cardiac specificity • Normal range within 24 hours
CAD – Angina Relationship Coronary Artery Disease / \ Stable Angina Acute coronary syndrome / / \ Unstable Angina > Myocardial Infarction ST-elevated MI Non-ST-elevated MI
Myocardial Infarction Acute Coronary Syndrome • Location correlates with coronary circulation involved • Inferior Wall – Right coronary artery • Anterior Wall – Left anterior descending • Lateral, posterior or inferior – left circumflex • Healing Process • Within 24 hours – leukocytes & enzymes • Third day – collateral circulation developing • 10-14 days – scar tissue is still weak • Vulnerable time – unstable state of healing + increased activity • 6 weeks – scar tissue replaces necrotic tissue • Normal myocardial tissue may compensate – ventricular remodeling – can cause late congestive heart failure