Download
1 / 46
560 likes | 1.12k Vues
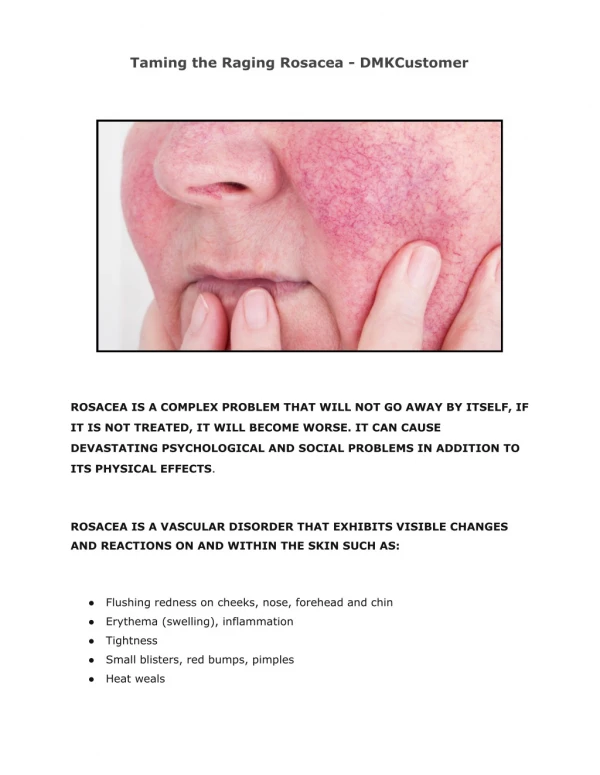
Rosacea. Cause unknown Aggravated by anything giving vasodilatation eg heat or caffeine Usually over 40yrs females, worse in males/Celts Onset gradual with papules and pustules on the cheeks chin mid forehead and tip of nose Erythematous background, often with associated telangiectasia.

E N D
Rosacea • Cause unknown • Aggravated by anything giving vasodilatation eg heat or caffeine • Usually over 40yrs females, worse in males/Celts • Onset gradual with papules and pustules on the cheeks chin mid forehead and tip of nose • Erythematous background, often with associated telangiectasia
Distribution Papules/pustules/erythema Nasolabial sparing
Can be unilateral Subtle telangiectasiae
Opthalmological problems • Up to 5% rosacea patients • Blepharoconjunctivitis • Lid hygeine, oral oxytetracycline for 6 wks if severe • Dry eyes – ocular lubricants • Chronic corneal inflammation and neovascularisation respond to low dose topical steroid (but risk of perforation) • Corneal perforation – keratoplasty
Prominent telangiectasiae suggests topical steroid use • Gross rosacea
Rosacea may persist and worsen • Exacerbated by anything causing flushing • Persistent red face with flushing may prove resistant to treatment • Remember carcinoid, facial fluishing but absence of other stigmata of rosacea.
Treatment • Mainstay broad spec antibiotics, mode of action unknown • Oxytetracycline 500 mgs bd • Rule of 1/3rds • 1/3rd better after 8 wks • 1/3rd better after 2nd or 3rd 8 wks of oxytet • 1/3rd need long term due to persistent relapse on cessation of treatment
Can use erythromycin or doxycycline • Antibiotics given for 2 months, should see improvement by 16 wks • Topicals • 0.75% metronidazole gel (Rosex) not as effective as oral antibiotics • Useful if get a flare of rosacea • Helpful to women candidiasis on antibiotics • Azaleic acid gel 15% • Clindamycin gel
58 trials, 6633 participants Doxycycline better than placebo 40mgs as effective as 100mgs Topical metronidazole Topical alazaic acid Further well-designed, adequately-powered randomised controlled trials are required Cochrane link
Treatment failure? • Most will have erythema/telangiectasiae ‘red face’ • Telangiectasiae can be treated by laser • Cosmetic camouflage • Referral for • classical rosacea not responding to treatment ?roaccutane • Significant rhinophyma – laser recontouring • Opthalmological rosacea
Seborrhoeic Eczema • Overgrowth of P. ovale (malassesia) in hair follicles giving a secondary eczematous response. • >30 yrs • males > females • Immunocompromised (HIV) • Gradual onset with erythema then scale usually in nasolabial folds • Often have scalp involvement – dandruff
Pink or red scaly ill defined patches, may become more acute with exudates. • Typical distribution • nasolabial folds, • eyebrows, • eyelashes (blepharitis), • ext auditory meatus • Scalp • Chest
Treatment • Tends to be persistent, fluctuating with weather, stress • Need to know how to look after the problem Pityrosporum ovale antifungals Inflammation topical steroids
Treatment • Treat yeast with imidazole eg ketoconazole • Nizoral shampoo twice weekly and cream bd • Maintainance shampoo once every 2 wks and cream in bursts every 2 weeks • 1% Hydrocortisone cream • 2% salicylic acid, 2% sulphur in aq. Cream • Lithium (ethalith) may be effective
SLE • A syndrome • Idiopathic or drug induced associated with autoantibodies • General symptoms • Fatigue • Fever • Weight loss • Malaise
Diagnosis: SLE requires 4 of 11 criteria • Malar rash • Discoid rash • Photosensitivity • Oral Ulcers • Polyarthritis involving more than 2 joints • Pleuritis or Pericarditis • Antinuclear antibody titer positive (1:40 or higher) • Titer over 1:320 is very suggestive • Renal disease • Neurologic disorder (e.g. Seizures, Psychosis) • Anaemia, neutropenia or thrombocytopenia • Anti-dsDNA, Anti-Sm positive, syphilis false positive
CDLE • Probably autoimmune affecting skin only not assoc with circulating antibodies • Precipitated and aggravated by sun • Middle aged and above • Gradual onset, patients notice scaly patches on the face • Absence of systemic symptoms
Prognosis, tends to persist until burnt out • Treatment • Potent top steroids – ie dermovate regularly • High factor sunscreens • Antimalarials – hydroxychloroquine if extensive or doesn’t respond • Retinoids • Immunosuppressants if severe and extensive
Light induced problems • Light sensitivity Juvenile Spring Eruption PLE • Sun damaged Solar elastosis AKs • DLE • SLE • Melasma
Actinic keratoses • Malignant potential • 0.1 – 10% • > 40yrs up to 40% population • May regress, remain static or undergo malignant transformation • Cryotherapy • Diclofenac • 5-fluouracil • Imiquimod • PDT
Treatment • Cryotherapy 5-15 secs freeze time • 3% Diclofenac (Solaraze) gel BNF: Apply thinly twice daily for 60–90 days; max. 8 g daily (carry on up the…………) • Imiquimod (Aldara). BNF: apply to lesion 3 times a week for 4 weeks; assess response after a 4 week treatment-free interval; repeat 4-week course if lesions persist; max. 2 courses Local reactions common on this regime – erythema, burning, ulceration, headache, flu symptoms
Field change actinic damage • Imiquimod weekly for 24 wks • 20 patients 28 wk trial once weekly for 24 wks assessed at 28 wks • 46.7% marked improvement • 6.7% improved on placebo • 5-FU (BNF) Apply thinly to the affected area once or twice daily; if possible, cover malignant lesions with occlusive dressing; max. area of skin treated at one time, 500 cm2 (23x23cm); usual duration of initial therapy, 3–4 weeks • Local irritation, severe discomfort (top steroid)