Download

1 / 56
890 likes | 4.17k Vues
Tetralogy of Fallot. Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery. Tetralogy of Fallot. 1. Definition Tetralogy of Fallot is characterized by underdevelopment of right ventricular infundibulum with anterior & leftward displacement

E N D
Tetralogy of Fallot Seoul National University Hospital Department of Thoracic & Cardiovascular Surgery
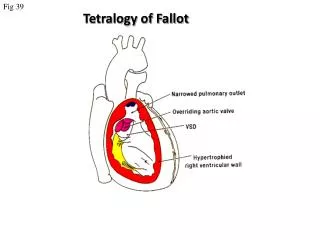
Tetralogy of Fallot • 1. Definition • Tetralogy of Fallot is characterized by underdevelopment of right • ventricular infundibulum with anterior & leftward displacement • (malalignment) of infundibular(conal, outlet) septum & it’s parietal • extension. This displacement of septum is associated with right • ventricular outflow stenosis & ventricular septal defect. • 2. History • Stensen : 1st description in 1672 • Fallot : Known tetralogy in 1888 • Blalock & Taussig : 1st surgical intervention in 1945 • Sellors & Brock : Closed valvotomy & infundibulectomy in 1948 • Lillehei & Varco : 1st repair by cross circulation in 1954 • Mayo group : 1st repair by pump oxygenator in 1955 • Kirklin : Conduit use for TOF+PA in 1966
Tetralogy of Fallot • Pathophysiology • Tetralogy of Fallot consists of a large VSD, RVOTO, aorta overriding the VSD, and right ventricular hypertrophy. • RVOTO leads to right-to-left shunting across a nonrestrictive VSD, resulting in adequate pulmonary blood flow and varying degrees of cyanosis. • It comprises 10% of CHD & the most common among the cyanotic defect(50%)
Pulmonary Infundibulum • Role & its function • The outlet portion of the right ventricle had not only a passive role in right ventricular contraction, and the peristaltic mode may be crucial to achieving a complete emptying of the right ventricular cavity. • The delayed opening of pulmonary valve might be more suitably explained by the peristaltic mode of function of right ventricle than by its intrinsic power • The pulmonary infundibulum ejecting the blood that it had accumulated at a time when the rest of the right ventricle was already relaxing.
Ventricular Interaction • RV & LV interaction -Cross-talk- • While the deeper layer of myocardial fibers are separated, there are shared superficial fibers that encircle the normal LV and RV. • Furthermore, in some forms of CHD, such as TOF, the deeper layers of RV and LV may be contiguous within the interventricular septum. • The function of the two ventricles is therefore linked, in both the structurally normal and abnormal heart.
Tetralogy of Fallot • Surgical morphology • 1. Right ventricular outflow tract • . Infundibulum, pulmonary valve, ring • 2. Pulmonary artery • . Trunk, bifurcation, distal PA, iatrogenic problem, • collateral blood flow • 3. VSD & conduction system • 4. Aorta, aortic arch & ductus arteriosus • 5. Right & left ventricle • 6. Coronary arteries • 7. Major associated cardiac anomalies • PDA, multiple VSD, A-V canal, ASD, AR
Tetralogy of Fallot • Surgical anatomy
TOF Aorta PA VSD VSD
Tetralogy of Fallot • Genetic syndromes & outcome • Approximately 10% to 15% of TOF patients carry a 22q11deletion (del22q11) and that 7% of TOF have trisomy 21 • Teralogy of Fallot patients with Alagille syndrome carrya mutation in JAG1 (jagged1 gene) and VACTERL, CHARGE,or other syndromes can be associated with TOF • Patientswith TOF and an associated genetic defect may face additional risk for primaryrepair; for example, if there is the need of extracardiac surgeryfor associated anomalies or because of immunodeficiency or alteredcompliance of the pulmonary vasculature.
Tetralogy of Fallot • Clinical features & diagnosis • 1. Clinical presentation • Cyanosis ; varies with severity of PS • CHF ; 10 % of patients in 2-3 months, and gradual increase in cyanosis • 2. Physical examination • Cyanosis of variable degree & clubbing, systolic ejection murmur • 3. Laboratory studies • Polycythemia , platelet depression, prolonged coagulation • 4. Chest radiography & electrocardiography • 5. Echocardiography, CT angio, MRI • 6. Cardiac catheterization & angiocardiography
Tetralogy of Fallot • Natural history • 1. Incidence : One of the most common CHD • 3~6/10000 births (5%~10% of CHD) • 2. Symptoms & survival : 25% death in 1 yr • 40% death in 3 yrs • 70% death in 7 yrs • 95% death in 40 yrs • 3. Hypoxic spell : Hyperactivity of infundibulum • in the 1st year of life & sudden • reduction of SVR • 4. Pulmonary artery thrombosis ; in severely polycythemia • 5. Pulmonary vascular disease ; rarely • 6. Genetic history ; more likely ( x 15 )
Tetralogy of Fallot • Operative indications • Diagnosis is generally an indication for repair. • 1. When asymptomatic & uncomplicated, repair is • deferred until 3 to 24 months of age. • 2. Initial shunting operation for symptomatic patient • less than about 6 months of age, & definitive • repair some time between 6 & 24 months of age. • 3. Early primary repair when the infant is importantly • symptomatic in the first 3 months. • 4. Early repair is advisable, particularly in the first • year of life
Tetralogy of Fallot • Aim of repair • First, the procedure must relieve the right ventricular hypertension ( PS ) by mobilizing, transecting, and infrequently, resecting parietal and septal extensions (bands) of the crista supraventricularis. • The aim of infundibular dissection is to increase the circumference of the infundibulum by enlarging each lateral recess in front of the conal septum • Second, the VSD must be closed completely while avoiding the conduction system • When the first criterion is met by a right atrial approach, it is considered the method of choice.
Tetralogy of Fallot • Operative techniques • 1. Evaluation • . Shunting vs one-stage repair • . Z-valve of pulmonary annulus • 2. Surgical approach • . Provide excellent exposure • . Avoid damage to coronary artery • . Avoid excessive muscle division in RV • 3. Details of repair • . Transventricular repair • . Transatrial & transpulmonary repair
Tetralogy of Fallot Systemic-pulmonary shunts • Various positions of the usual systemic-pulmonary • arterial shunts for augmenting pulmonary blood flow
Systemic-Pulmonary Shunts • Via median sternotomy
Tetralogy of Fallot • Anatomy • Anatomic substrate of repair from right ventricular approach
Tetralogy of Fallot • Anatomy • Anatomic substrate of repair from right atrial approach
RVOT Reconstruction • Principles • The diameter of annulus with a Hegar dilator that passes snugly but not tightly through it. • Generally, a transannular patch should not be placed when Z value is larger than -3. • When a polyester tube is used, one is selected whose diameter corresponds to a Z value of 0 to +2. • The patch when properly trimmed, its convexity is ensured in all direction, as is a relatively square cut of its distal end. • To widen the LPA stenosis, a rectangular piece of pericardium is cut about one and a half times wider than the apparent diameter of the LPA and about one and a half times longer than the incision in the LPA.
RVOT Reconstruction • Application of monocusp patch • Transannular patching is often necessary for reconstruction of right ventricular outflow tract obstruction, but it leads to transvalvular regurgitation. • Acute pulmonary valve regurgitation of higher degrees impairs right ventricular function, and seems to be associated with increased perioperative mortality. • Regurgitation fraction after reconstruction is dependent on the length of the monocusp patch relative to the length of the hypoplastic pulmonary root. • The best result was obtained with a monocusp patch roughly two times as wide as the hypoplastic pulmonary root
RVOT Patch Widening • Principles • The width of the patch across the pulmonary annulus must be generous enough to eliminate most of the gradient. • It is better to accept a mild to moderate gradient than to create wide open pulmonic insufficiency. • The new annulus diameter should not be much greater than the Z-zero pulmonary annular size for the patient. • The toe of the patch must be oval or square to minimize the risk of subsequent anastomotic stenosis
Tetralogy of Fallot • Surgical repair
Tetralogy of Fallot • Operative technique • The rectangular patch when properly trimmed, its convexity is • ensured in all direction, as relatively “square cut” of its distal end.
Tetralogy of Fallot Patch enlargement • Extension of a pulmonary arteriotomy onto the left • pulmonary artery and correct patch configuration
Tetralogy of Fallot RVOT reconstruction(1) • Monocuspid valve
Tetralogy of Fallot RVOT reconstruction(2) • Monocuspid valve may be attached to the pericardial roofing patch. • The cusp diameter is fashioned somewhat larger than the planned • roofed RV outflow.
Tetralogy of Fallot RVOT reconstruction(3) • It is cut more or less circular and sutured to the patch when • the latter suturing from distally reaches the valve annulus.
Pulmonary valve saving Tetralogy of Fallot
Tetralogy of Fallot • Pulmonary valve saving
Pulmonary valve-sparing Tetralogy of Fallot (A) Pulmonary arteriotomy. (B) Autologous pantaloon pericardial patch. (C) Completed pulmonary artery pantaloon patch.
Tetralogy of Fallot • Postoperative care • Patients have a tendency to increase their interstitial, pleural, & peritoneal fluids early postoperatively. • The hemodynamic state is assessed continuously and management constantly reviewed. • Care lest loss of intravascular plasma to extravascular spaces produces undesirable hemoconcentration early postoperatively. • Bleeding because of preoperative polycythemia and depletion of many clotting factors, extensive collateral circulation, and damaging effects of CPB. • Body weight is followed closely because transient fluid retention is common, especially transannular patch.
Postrepair RV Pressure • Factors of PRV/LV • Pulmonary arteriolar resistance • Size of the LPA and RPA • Presence & severity of localized or segmental stenosis or incomplete distributions of pulmonary arteries • Residual pulmonary trunk or RV outflow obstruction • Increased flow through RVOT by residual shunting and by pulmonary regurgitation
Tetralogy of Fallot • Special situation & controversies • Rationale for use of postrepair PRV/LV • Initial palliative operations preferred median sternotomy in all age • Palliation by beta-adrenergic blockade 2-6mg/kg/day • Initial palliation by balloon valvotomy • Monocusp valves beneath patches
Tetralogy of Fallot • Neurodevelopmental impairment • Neurodevelopmental impairment is known in children afterpalliative or corrective surgery for cyanotic heart diseasebeyond infancy • Preoperative impairment,however, due to prolonged chronic cyanosis with thromboembolicor septic brain damage, should be markedly reduced in Fallotpatients without preoperative complications and operated onduring infancy • Influences of preoperative & perioperativeconditions with elevated circulating levels of proinflammatorycytokines in hypoxemic patients might bealso in part responsible for damage to the brain
Tetralogy of Fallot • Surgical results • 1. Survival • Early death ; recently less than 1% • Time-related survival ; good • 2. Modes of death ; subacute heart failure • 3. Risk factors for premature death • 4. Heart block, arrhythmia, sudden death • 5. Right ventricular function & aneurysm • 6. Residual outflow tract obstruction • 7. Left ventricular function & functional status • 8. Residual VSDs & bacterial endocarditis • 9. Pulmonary function • 10. Reoperation & other reintervention
Postrepair Tetralogy of Fallot Risk Factors for Premature Death • 1. Very young age at repair • 2. Older age at repair • 3. Severity of “annulus” hypoplasia • 4. Size of pulmonary artery • 5. Transannular patch • 6. Postrepair pRV/LV • 7. Previous palliative operations • 8. Multiple VSD ; 1-3% • 9. Coexisting related cardiac anomalies • ECD, Down syndrome, MAPCA • 10. Other risk factors ; small LV
Primary Repair of TOF • Advantages in early infancy • 1. Avoidance of the risk of palliative operation • 2. Prevention of shunt-induced PA stenosis • 3. Obviation of the need to take down shunt • 4. Early relief of RV hypertension • 5. Avoidance of excessive LV volume load • 6. Elimination of Rt-to-Lt shunting across VSD
Tetralogy of Fallot • Benefits of early complete repair • Normal growth and development of organs • Elimination of hypoxemia • Less need for extensive right ventricular muscle excision • Better late left ventricular function • Decreased incidence of late dysrrhythmias
Tetralogy of Fallot • Late problems after repair • Late death, sudden cardiac death • Redo operation • Aortic root dilation, AR and AVR • Residua, sequelae ( PR, TR, RVOTO, VSD) • Arrhythmias (SSS, CAVB, AF, AFL, VT) • Impaired cardiopulmonary performance • Impaired autonomic nervous system • Ventricular dysfunction (RV, LV failure) • Infective endocarditis
Results after TOF Repair • Risk factors for late death • Residual VSD • Residual RV outflow stenosis • Severe PR • Severe TR • Older age at repair • Previous Potts, or Waterston shunt
Tetralogy of Fallot • Considerations in adult • Collaterals or preexisting shunts lead to increased pulmonary blood flow, and togetherwith myocardial hypertrophy and myocardial hypoxia, they leadto reduced biventricular function. • Impaired ventricular function,severe hypoxemia, and tricuspid regurgitation are associatedwith a higher operative mortality, whereas the influenceof age at the time of operation is controversially • Cyanosis and erythrocytosis leadto thrombosis, infective endocarditis, stroke, brain abscess,myocardial fibrosis, impaired ventricular function, and multiorgan dysfunction could be the mostimportant risk factor
Tetralogy of Fallot • Risk factors in adult • Prolonged cyanosis causes myocardialand other organ dysfunction • Heart is chronically volumeoverloaded, especially in previous palliativeprocedures and aortopulmonary collaterals • Bleeding tendency is also important • The noncompliant hypertrophic adultright ventricle seems to tolerate pulmonary valve regurgitationpoorly, the second significant predictor of early mortalitybeing the need for right ventricular outflow patch • The native pulmonary valve is of course preserved andrepaired whenever possible
Results after TOF Repair • Causes of sudden death • Bradyarrhythmias such as complete AV block, bifascicular block, SSS • VT and residual RVOTO and RV dysfunction • Complex ventricular arrhythmias by Holter monitoring • Monomorphic VT and severe PR, peripheral PS, RV dilation, QRS duration more than 180ms
Arrhythmia & Sudden Death • Approaches after TOF repair • QRS Easy to measure Reflects RV size Dynamic nature, QRS change important New QRS cutoff values for contemporary cohorts • QT dispersion Refines risk stratification Less dynamic May reflect initial ventriculotomy scar/ VSD closure
Sudden Cardiac Death • Mechanisms of SCD after TOF repair 1. SCD & sustained VT in common Electrophysiologic profile Long QRS QRS change QT dispersion Hemodynamic substrate PR moderate/ severe Cardiomegaly/RV dilation 2. SCD different from sustained VT patient; olde age at repair 3. Overlap between AF/AFL/sustained VT & SCD
Tetralogy of Fallot • Causes of ventricular dysfunction • LV dysfunction • Secondary to inadequate myocardial protection during initial repair • LV volume overload due to longstanding palliative shunt or residual VSD • Myocardial fibrosis because of longstanding cyanosis or RVOTO • RV dysfunction • Residual RVOTO • Longstanding PR , TR • Surgical scar, RV and /or RVOT patching, aneurysm
Autonomic Nerve System • Impairment after TOF repair • Reports demonstrating depressed heart rate variability and baroreflex sensitivity suggest that the autonomic nervous system change may also involved in arrhythmogenesis • Also depressed heart rate was observed in repaired TOF patients during exercise and pregnancy
Aortic Root Dilation • Late after TOF repair • Shunt to repair time interval • Male gender • Pulmonary atresia • Right aortic arch • Aortic regurgitation • LV enlargement
Tetralogy of Fallot • Mechanisms of aortic root dilation • Underlying abnormality • Reciprocal morphogenesis of Aorta/PA • Increased flow from both ventricle • Abnormal morphology • Intrinsic medial abnormality • Acquired hemodynamic influences • Increased flow through aorta • Increased volume/ pulsatility • Infective endocarditis • Surgical damage • Residual VSD
Pulmonary Artery Lesions • After TOF repair • Incidence of reoperation ; 5~14% • Reasons of restenosis of RVOT 1. Restricted growth of RVOT 2. Miscalculated sizing of RVOT 3. Angulation & stenosis of LPA 4. Compression/angulation of PA caused by RV hypertrophy or dilation 5. Most common location is pulmonary bifurcation or origin of PA branch.