Download
1 / 42
420 likes | 538 Vues
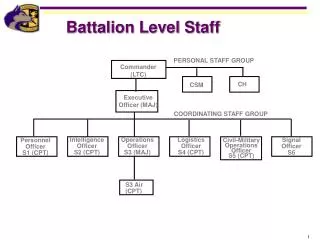
Consultative Staff Support Group. Howard Gruetzner, M.Ed., LPC Education and Family Care Specialist Alzheimer’s Association, North Central Texas Chapter Author, Alzheimer’s: A Caregivers Guide and Sourcebook , 3 rd Rev, 2001. Objectives.

E N D
Consultative Staff Support Group Howard Gruetzner, M.Ed., LPC Education and Family Care Specialist Alzheimer’s Association, North Central Texas Chapter Author, Alzheimer’s: A Caregivers Guide and Sourcebook, 3rd Rev, 2001
Objectives • Describe care in relation to dementia (research-based). • Describe group principles as they apply to the consultative staff support group. • Describe care principles as they apply to the consultative support group.
Recommendations on Staff Support For Dementia Care • Need Staff Support that prevents stress and burnout • Training on ways of dealing with persons with dementia and their behaviors • Improve communication skills with persons with dementia
Recommendations on Staff Support For Dementia Care • Increase understanding of resident’s physical and social needs so that interpretation of behavior shows better understanding of causes and greater tolerance for range of behaviors.
Recommendations on Staff Support For Dementia Care • Training nurse trainers to provide leadership and serve as role models • Refresher courses for training that have been done so that positive effects can be maintained.
Recommendations on Staff Support For Dementia Care • Support from Management for new practices to resolve potential conflict between task-focused practice and promotion of individualized, client-focused care.
Recommendations on Staff Support For Dementia Care • Refresher courses for training that have been done so that positive effects can be maintained. • Groups to provide nursing assistants with support and the development of coping skills should be utilized more widely
Recommendations on Staff Support For Dementia Care • Education with peer support found that staff who received both were more likely to feel satisfied with their knowledge about dementia and confidence when working with residents with dementia
Kitwood’s (1997)theory of personhood in dementia Personhood defined As a standing or status that is bestowed upon one human being by others, in the context of relationship and social being. It implies recognition, respect and trust (Kitwood, 1997, p. 8)
Personhood Personhood is not the ‘property’ (Kitwood & Bredin, 1992) of the individual, but is a status that can only be provided or assured in the context of a mutually recognising, respecting and trusting relationship.
Person-Centered Care • Based on the fundamental premise that each person is unique • Care should be based on each individual’s strengths, interests, and needs
Consultative Staff Support Group The Consultative Staff Support Group concept has been utilized in two different facility settings: • Meridian Manor for staff on their secure dementia unit who could attend. • Wesley Woods Alzheimer’s Care Center and limited to staff on the facility’s behavior unit.
Meridian Manor The meetings were on a monthly basis that covered six months. Certified Nurse Aides and other staff that included nurses and activity persons attended. Several of these meetings were conducted during a period of time without a Director of Nurses on staff.
Wesley Woods Alzheimer’s Center The majority who attended the monthly groups were certified nurse aides but nurses did attend a few of the meetings. The group helped introduce the beliefs of the care culture for new staff who attended.
Consultative Staff Support Group • Recognizes the need for all staff, and especially direct care staff, to develop appreciation for the primary importance of relating to persons and not tasks • Without relationship characterized by security and trust the tasks are more difficult to provide
Consultative Staff Support Group • Relationship is based on understanding of person before dementia and how dementia has affected that person’s expression of needs and preferences • Needs and problems are never interpreted solely as result of dementia
Concept of Group The consultative support group draws from the concepts of support groups, staffing and case consultation. It was led by a consultant with clinical, research, management and supervisory experience.
Principles Emphasized • Group time limited to 1 hour and this was always honored so that staff backup and going to the next shift not disrupted. • Combination of support group and case consultation approaches to care and coping for staff facilitated and led by professional consultant to the facility.
Principles Emphasized • Staff always encouraged at the beginning of each group to talk about what they would like to discuss: something that bothered them or idea they wanted to discuss.
Principles Emphasized • This empowered them as staff and as persons. If they did not have something I would always have some questions or situations to explore with them- some of these presented by staff in prior groups.
Principles Emphasized • Groups were open to either staff members from a specific unit or jobs, e.g., behavior or dementia unit; staff without management or supervisory roles.
Principles Emphasized • Staff members working on a specific unit- like participants of other support groups- by definition share experiences though they may not share the same view of the experiences.
Principles Emphasized • They may frame problems differently and thus see different and more successful approaches that can be shared with coworkers. They can be helpful to one another by sharing such knowledge, encouraging one another, talking about their normal feelings without fear of judgment.
Principles Emphasized • The combined concepts- mutual support and focused problem-solving- teach and practice a broad spectrum of coping approaches for staff to utilize in resident care, coping with stressful situations, and working together- often with the same residents. Promotes the idea of team and belief that staff can share support and solutions with each other.
Principles Emphasized • Special attention was given to the cognitive beliefs or biases staff inadvertently represented by their comments that created barriers to the care they were providing because of the perception they had of the person.
Principles Emphasized • Examined whether dementia was the biggest factor of if the behavior was driven by other premorbid factors like personality or likes and dislikes. • Helpful to have staff discuss beliefs explaining the behavior and then question how helpful such beliefs were in relating to the person and the task.
Principles Emphasized • Causes of dementia-related behavior problems were viewed as having multiple sources. This gave staff more factors to consider when looking at solutions or more fitting approaches to problem solving. This approach also helped staff see the person and not the behavior as the person.
Principles Emphasized • Frequently staff members had similar perceptions of the problems but had other ways of dealing with the problems in managing behavior or interacting with family members.
Principles Emphasized • Promoted the belief that we choose to deal with problems in ways they make them better or worse. We do that by how we choose to adapt even when there seems to be no good choice.
Principles Emphasized • The group emphasized the value of the staff person beyond the role of professional caregiver. This appreciates the caregiver part of staff roles- meaning they need to learn how to care for themselves to be emotionally available to persons with dementia and have a life outside the job.
Principles Emphasized • Promoted the belief that we choose to deal with problems in ways that make them better or worse. We do that by how we choose to adapt even when there seems to be no good choice.
Principles Emphasized • Staff was challenged to see tasks in the context of persons rather than the task as the sole focus of contact with the person. • The relationship with the person is viewed as the most important part of the contact so task could occur in the context of the relationship rather than be the sole reason for the contact.
Principles Emphasized • Behavior was generally interpreted as a source of meaning and understanding of the person that could lead to a helping response rather than being framed only as a problem.
Illness orientation Loss abilities-what person cannot do Disability caused by dementia Person-Centered Retained abilities, what person can do Strengths, interest, skills Longstanding traits, abilities, preferences, experiences, habits New vs. Old Culture of Dementia Care: Focus Old Culture New Culture* Revised by M. Smith(2005) from M. Smith & K.C. Buckwalter (1993), Geriatric Mental Health Training for Hartford Center of Geriatric Nursing Excellence, College of Nursing, University of Iowa
“Nothing can be done “Incurable” “No hope” Person-first, i.e., person-centered Continued meaning in life Ability to enjoy life retained New vs. Old Culture of Dementia Care: Attitudes Old Culture New Culture
All caused by disease Brain Changes due to dementia & progression Unmet needs Enduring traits & habits Stress Environmental factors New vs. Old Culture of Dementia Care: Behaviors
All Behaviors caused by disease Behavior = COMMUNICATION discomfort, e.g., pain distress, e.g., fear and anxiety New vs. Old Culture of Dementia Care: Behaviors Old Culture New Culture
Negative Terms for BEHAVIORS Disruptive Difficult Aggressive Behavior as SYMPTOM Behavioral and Psychological Symptoms of Dementia (BPSD) Need-Driven Dementia-Compromised Behaviors (NDB) New vs. Old Culture of Dementia Care: Labeling Old Culture New Culture
Negative Terms for PERSON “Hitters” “Feeder” Demented Person Behavior as SYMPTOM Behavioral symptoms, or just behaviors Person-Centered Person with Dementia (PWD) Person New vs. Old Culture of Dementia Care: Labeling Old Culture New Culture
“Manage” behaviors “Control” person who is likely to “cause trouble” Contain behaviors and/or disallow negative influence on others in environment Understand & respond vs. “manage” or “control” Problem-solve about meaning of behavior Why here? Why now? New vs. Old Culture of Dementia Care: Interventions Old Culture New Culture
“Manage” behaviors Who has “problems”? Promote function and comfort Engage in pleasurable activities Distract, reassure, comfort New vs. Old Culture of Dementia Care: Interventions Old Culture New Culture
It’s Important to Know What Disease a Person Has, But It’s More Important to Know What Person the Disease Has. ---- Dr William Osler