Download
1 / 38
380 likes | 509 Vues
Improving Communication Between Healthcare Providers Outside and Within Hadassah: Use of Academic Detailing to Overcome Barriers. Presentation to Hadassah Board Quality Committee January 11, 2012. Alyssa Hochberg, BSc Meir Frankel, MD Lois Gordon, MPH Mayer Brezis, MD MPH

E N D
Improving Communication Between Healthcare Providers Outside and Within Hadassah: Use of Academic Detailing to Overcome Barriers Presentation to Hadassah Board Quality Committee January 11, 2012 Alyssa Hochberg, BScMeir Frankel, MDLois Gordon, MPH Mayer Brezis, MD MPH Center for Clinical Quality & Safety Hadassah Hebrew University Medical Center
2010 Project: Survey of 100 patients hospitalized while taking 5 or more medications Chaos Waiting for Bad Luck? Medication Reconciliation Should Be Mandatory In 97%, there was an error in the prescription in hospital or at discharge On average: 3 errors per patient 1% potentially life-threatening Roni Cohen, B.Sc., InbalYifrach-Damari, M.Sc.* Dr. Meir Frankel, Prof. Mayer Brezis *Clinical Pharmacist, Pharmacy Division Hadassah-Hebrew University Hospital, Jerusalem, Israel Pharm-D student, School of Pharmacy, Hebrew University With Help From Joint Commission International
Medication Errors • Medication errors are the fourth leading cause of death or major permanent loss of function in hospital patients. • The majority of problems with patient safety occur during the transition from one care setting to another. • Ambulatory-hospital lack of communication is responsible for 50% of medical errors.
The Challenge of Improving Transition of Care Hospital Community Quality of Transition Quality of Cycle of Care Continuity of Care
Improving Communication Between Healthcare Providers Outside and Within Hadassah: Use of Academic Detailing to Overcome Barriers Presentation to Hadassah Board Quality Committee January 11, 2012 Alyssa Hochberg, Lois Gordon, Dr. Meir Frankel, Prof. Mayer Brezis Hadassah Center for Clinical Quality and Safety Hebrew University of Jerusalem
Introduction Follow-up care is a weak link in the chain of quality of patient care, and lack of accuracy in information transfer between caregivers, in the community and in hospitals, can result in errors that can be life-threatening. Attempts to implement communication via computerized systems between health funds and hospitals have encountered technical and logistical problems, as well as a lack of cooperation on the part of physicians.
Introduction For example: during the past two years, a computerized communications system has been established between Hadassah and the Maccabi and Meuhedet Health Services. Via this system, hospital-based doctors can obtain information on the diagnoses, blood tests and routine medications of their hospitalized patients.
Introduction Notification has been sent to medical staff working with these communication systems, but its use has been limited. Attempts by Meuhedet to create similar computerized systems in a number of their emergency facilities in Israel have met with a similar fate. In order to implement the use of such computerized systems, keeping in mind the limitations that have prevented their widespread use, a decision was made to use ACADEMIC DETAILING as a tool.
Introduction Academic Detailing The “educator” for this method of academic detailing is a professional, such as a pharmacist, nurse, doctor or medical student, who acts as a promoter for the improvement of patient care. This educational method is based on medical facts, supports patient safety, takes into account cost-effectiveness, and is directed towards improving the quality of medical care. A key component of academic detailing is its financial independence from the pharmaceutical industry!
Introduction Academic Detailing • Academic detailing is comprised of education through academic promotion directed towards physicians in emergency rooms. • Research has shown that this method is practical, efficient and safe, particularly when combined with process supervision and appropriate feedback from the medical staff. It is an excellent means of implementing specific positive behavior patterns among hospital staff.
Introduction: Academic Detailing This method, introduced by Jerry Avorn (Harvard), Avorn and Soumerai. Improving drug-therapy decisions through educational outreach — A randomized controlled trial of academically based detailing. N Engl J Med 1983; 308:1457-1463 Avorn and Soumerai. Principles of educational outreach ('academic detailing') to improve clinical decision making JAMA. 1990;263:549-556 has succeeded in effecting changes such as: • Reducing overuse of wide-spectrum antibiotics Solomon D.H. et al, Academic detailing to improve use of broad-spectrum antibiotics at an academic medical center. Arch Intern Med 161;2001;1897-1902 • Reducing overuse of antidepressants for elderly van Eijk M.E.C. et al, Reducing prescribing of highly anticholinergic antidepressants for elderly people: randomised trial of group versus individual academic detailing. BMJ 322;2001;1-6. • Reducing medication errors Wortman S.B., Medication reconciliation in a community, nonteaching hospital. Am J Health-Syst Pharm 65;2008;2047-2054
Implementing the Use of Computerized Communication Systems Intervention Program Using Academic Detailing
Computerized Communication Between Hadassah & the Community In January 2011, a cooperative effort between Hadassah and the Meuhedet Health Services began. A computerized system was set up for obtaining information on patients arriving at the emergency room or hospitalized at Hadassah. With the establishment of the system, notification was sent to all hospital staff. However, over a four-month period, use of this computerized system remained marginal.
Computerized Communication Between Hadassah & the Community Since 2009, there has been similar cooperation between Hadassah and the Maccabi Health Services. A computerized communications system was established to enable receipt of information on Maccabi patients hospitalized at Hadassah. Use of this system was also very marginal.
Implementing the Use of Computerized Communication Systems: The Intervention Program The use of academic detailing: this method is comprised of education through academic promotion directed towards physicians in emergency rooms. In practice: promotional activity on the part of a medical student, directed towards doctors in the emergency rooms of Ein Kerem and Mount Scopus hospitals included: general explanation of the system, advantages, and individualized demonstrations geared towards helping ER doctors use the program effectively.
Implementing the Use of Computerized Communication Systems: The Intervention Program The intervention included: Speaking to doctors individually Evaluating their familiarity with the system Understanding their attitude towards using the system: advantages, barriers to use and suggestions for improvement
Printing additional information from the system and adding it to patient files with a sticker to flag the information obtained from the system
Posting informational signs near the computer stations at the hospital, to encourage use of the system • Sending an e-mail to all hospital physicians about the computerized program
Implementing the Use of Computerized Communication Systems: Methods Data gathering is comprised of both quantitative and qualitative aspects. Quantitative research: evaluating the change in the proportion of entries into the system before, during and after the intervention (prospective study). Qualitative research: based on the responses of the doctors themselves and serves as a means of understanding the advantages and disadvantages of the system, barriers to its use and suggestions for improvement.
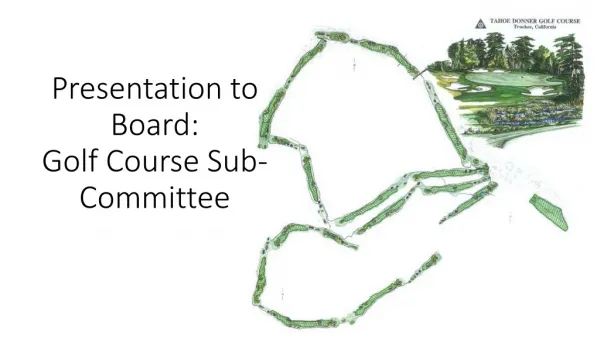
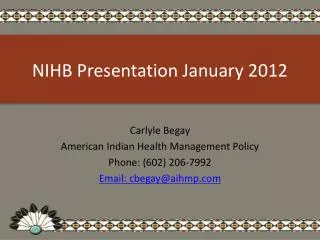
Preliminary Results From a quantitative perspective, an initial analysis indicates that a significant increasein the number of system entries has been observed, close to and following the intervention, as indicated in the following graph…
email & outpatient clinics intervention: academicdetailing E I N K E R E M signs & email communication system with Meuhedet ER visits 2011: Ein Kerem
MOUNT SCOPUS email & outpatient clinics intervention: academicdetailing signs e-mail ER visits 2011: Mt. Scopus
Qualitative Results During the initial individual meetings of the medical student with 97 doctors, it became clear that: • 51% do not use the computerized program in the emergency room • 14% have used it once or twice • 24% have used it several times • 10% have used it only “when relevant” (without specifying the number of times) • 27% did not know about the existence of the system
Qualitative Results 47%of the doctors received a complete explanation of the program and its link to health fund records 37% of the doctors witnessed a demonstration of the program 35%of the doctors thought that they would use the program after receiving an explanation/demonstration.
Important Observations Made by the Doctors Approached Positive reactions: great idea, technically simple, works beautifully in the ER Significance of the system: identifies medication given or auxiliary tests performed at health fund facilities; useful when there is lack of information (regarding creatinine levels or previous ECG); “very useful” and improves patient care Barriers encountered: “there’s enough information from other sources”; “we’re not used to using the system”; “don’t use system because of time constraints in the ER”; “we didn’t manage to access the system from the ER”; “the link is not user-friendly.”
Important Observations Made by the Doctors Approached Suggestions for improvement: • Updating and organization of patient medications in the system • Automatic copy/paste of information from health service records into Hadassah’s computer system • Allow entry into the system from outpatient clinic computers • Allow entry into the system for clinical pharmacologists and nurses • In addition, many doctors emphasized the need for access to Clalit Health Services records
Research still lacks a long-term perspective Change in quality of care as a result of an increase in system usage was not examined. However, an Israeli study conducted in 2010 indicated that use of a computerized communications system with Clalit Health services reduced the number of radiological examinations and was linked to improvement in certain select quality parameters.* Some doctors refuse to even be informed about the system/use it (although they were a minority). *Nirel N. et al, OFEK virtual medical records: an evaluation of an integrated hospital-community system. Harefua2011Feb;150(2):72-8, 209. Limitations of the Study
Conclusions Current results indicate that this intervention resulted in increased use of the computerized system, raised suggestions regarding improvement, and helped in understanding doctors’ attitudes towards using the system. Technology benefits from promoting appropriate usage! Academic detailing is an interesting and promising method for understanding barriers, changing behavior of hospital-based clinicians and implementing a new and useful computerized tool that can greatly assist doctors.
Acknowledgments Dr. Rosenblum and staff, Department of Information Systems, Meuhedet Health Services Prof. Yosef Karako and staff, Department of Information Systems, Macabbi Health Services Ms. Efrat Simon and staff, Department of Information Systems, Hadassah Medical Center Dr. Kobi Assaf and staff, ER Hadassah Ein Kerem Dr. Stalnikovich and staff, ER Hadassah Mount Scopus
Further Steps • Extend “IT connectivity” to other sick funds (Clalit & Leumit) • Continue monitoring use; boost academic detailing as needed • Introduce formal medication reconciliation at all transitions • Develop other “transition-of-care tools” to improve the routine teamwork among departments • Recheck error rates
Some speciality clinics X-rays CT, US Many speciality clinics Hemodialysis Primary physician Multi-disciplinary clinics Breast cancer screening (mammography, biopsy, etc.) Endoscopy, Bronchoscopy Simple lab tests Simple surgeries Ophthalmology Plastic surgery etc. Day care Hematology Heart failure High-technology labs Between Hospital and Community:More Than Just Medications… Hospital Radiology (CT, US, MRI) Gastro/Colonoscopy Expert consultation Day care Echo, Holter Bronchoscopy Hemodialysis Surgery Angiography Multi-disciplinary clinics (diabetes, breast, etc.)
Department ER Department B Department A Department ICU OR Department OR ICU Institutes (Cardiology, Gastroenterology, Pulmonology, Invasive Radiology etc.) Department Department Hemodialysis Intra-hospital Transitions