Download
1 / 57
570 likes | 730 Vues
Why We Make Mistakes. Jeffrey Young, MD Senior Associate Chief Medical and Quality Officer Professor of Surgery Director, UVa Trauma Center University of Virginia Health System. First step in understanding error How do we carry out diagnosis and treatment?

E N D
Why We Make Mistakes Jeffrey Young, MD Senior Associate Chief Medical and Quality Officer Professor of Surgery Director, UVa Trauma Center University of Virginia Health System
First step in understanding error How do we carry out diagnosis and treatment? Where are the opportunities for safety? Understanding Clinical Care
Knowing how to accurately assess the state of a patient What data and actions are necessary to get an accurate assessment Knowing the significance of the data reflecting the patient’s current state Matching the patient’s state to the correct schema Mentally testing and activating an acceptable action plan Follow-up Cognitive skill
Medical education Even problem based curriculums are not truly tactically oriented Issue – data- analysis- action- reassessment Differential diagnosis Look at data and create diagnosis list based on characteristics of conditions and their relation to the data you currently have available Then look at list and decrease number of diagnoses until you are left with one Background
We are not trained to rapidly assess a situation, look at the key elements, discard less important inputs, create an action plan, implement it , and see if it worked Military does this very well, as do other high risk jobs (aviation, etc.) Tactical Assessment
Do a thorough history and physical examination Chief complaint HPI ROS Medications Allergies Physical Exam Assessment Plan Current Process
Signs and symptoms lead to potential diagnoses Diagnoses lead to investigation Through investigation diagnoses are supported or discarded You are left with your most likely diagnosis Then you initiate a treatment plan Assessment/Plan
Definitive treatment delayed until all possibilities are entertained and evaluated There is concern that aggressive early intervention can lead to overtreatment, incorrect therapies, or complications of medications and procedures Paradigms
Some patients have time for thoughtful evaluation Some do not First cause of error: not making the above characterization of the patient correctly Bottom Line
Knowing the indications for a test or procedure Knowing how to safely carry out the action, and all possible adverse events related to that procedure Insuring backup and help if needed Monitoring the patient during the procedure Correctly interpreting the results of the procedure Following up to insure absence of adverse event Technical Skill
Can not carry out technical act, nor action plan without other competent individuals or processes Need to know how to engage the care team Advice members of goal, path to goal, alternative paths if they arise, Framework for communication Checklists and Time outs CRM principles during action plan Follow-up Teamwork
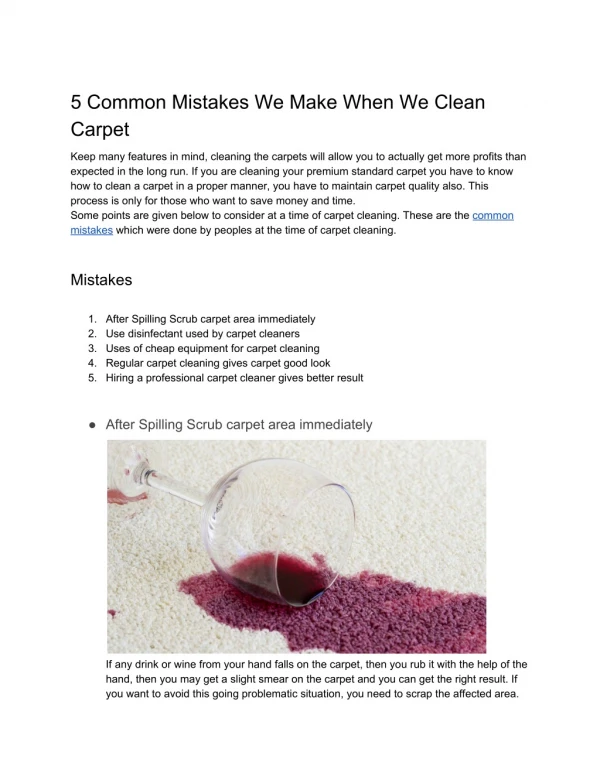
Intern is on call and at 1AM nurse calls: “ Mr. Smith who had a stent placed for a AAA today is having some belly pain and his temp spiked to 38.7C” Example
Intern “Well…how bad does his belly hurt?” “He had his procedure today, I’m sure he just has some atelectasis, make sure he uses his incentive spirometer” “Thanks for the call” Opportunity of Error
Have we given that intern the tools to ask the right questions and do the right things? Have we prepared him to fail in this case or succeed? Would a better understanding of how people make errors improve his chances of success? Can we learn from other high risk industries? Error
Novices Novices (or people inexperienced in that domain) do not yet have the experience and knowledge to make correct decisions They don’t know what can go wrong Don’t know the cues Don’t even know what data to look for Thus they must depend on an overall philosophy or mindset toward events to guide their decisions If that mindset is dangerous, bad care will result Experience and Error
Experts When you are an expert, you’ve gained the experience and knowledge to properly make decisions You know what data is essential and what is extraneous You can look for cues that put you down the correct path Can we teach this? Or do you have to live it? Experience and Error
Slips Failures to properly adjust tasks that require little conscious attention to the characteristics of a new situation Without thinking, ordering an adult dose of a med for a child Correction Make it difficult to do the wrong thing Error requires more steps and positive affirmation “Do you really really want to format C:?” Types of Errors
Lapses Failures of memory that cause tasks not to be done Common in task overload or distraction How to avoid? Train in high intensity situations Clear pre-arranged plans that require little creative thought and may not be perfect, but are SAFE Reminders Same corrective actions as for slips Types of Error
Mistakes The selection of incorrect actions by misclassifying a situation or failing to take into account all relevant factors in a decision Evaluating for nausea and vomiting but not taking into account new onset DM as a cause Attributing cold symptoms to the URI and not realizing degradation in cardiac function is the cause Perfect execution of incorrect plans distinguishes this from lapses and slips Errors
Assumptions It must be OK or someone would say something Generalizations Didn’t happen last time, why should it happen this time? (translation; I got away with it last time….) Successful folly is folly nonetheless (Jim Hurst, MD) Pushing a bad system to the limits Without working on making the system better Error Generators
Laziness (not that common) And number 1(‘s)! Too little FEAR that things can go wrong “Fear does the work of reason” – Winston Churchill quickly and with very little warning. Making CERTAIN that the conditions are stable or improving before moving on Too little FEAR that you don’t know everything Error Generators
Incorrect triage of problem Problem more serious than most people realize Insufficient fear of being wrong Practitioner has not seen enough clinical situations to know all possibilities Buggy knowledge – they fill in their knowledge gaps with generalizations No follow-up Almost all major disasters can be averted by simply going back and reassessing the patient Common Causes of Clinical Error
Lack of cognitive understanding of condition or state by all practitioners (Most common cause of adverse events I see) Team does not have enough experience or know enough to realize what is going on with patient Patient in ectopic units Specialists not available Patient at low capability facility (don’t understand who is at risk) Error Recovery
Very complex issue Systems, education, decision making, communication New knowledge, new techniques and procedures Information systems Error Prevention
Schema (what is the mindset you are using with this patient?) You actually decide what “kind” of patient you have very rapidly (almost instantly), but you may not realize it Visualize care plan In mind, can I see this patient going home the way they look now? Does the patient look like the typical patient who is admitted for this type of problem? What Can We Learn From Studies of How Experts think?
Very few major disasters result from a single error “Tactical catastrophes are rarely the outcome of a single poor decision. Small compromises incrementally close off options until a commander is forced into actions he would never choose freely” – Nate Fick
Situations Where Error May be Unrecoverable Tenerife: March 27, 1977 Worst Aircraft Accident in History Factors: Inadequate technical skills of ATC Suspect plan (?) Experienced pilot (top airline pilot at KLM) Fog No ground control radar CRM Stepped on transmissions No warning system for active runway
Cognitive Decision to take off Decision to place both planes on runway Decision to refuel Technical No ground radar Communication equipment inadequate Teamwork Cockpit and control tower teams Errors
This accident (more than any other) changed the culture of air safety To be honest, we have not yet had such an incident in medicine (IOM report?) When people realized even the most experienced pilot could make egregious error, conclusion reached that human performance must be enhanced with safety measures Sometimes we just do real stupid things Tenerife
“Good judgment comes from experience, and experience comes from bad judgment “ “Luck is not method, and neither is hope. Hard work is.” Can we produce safe doctors with decreasing clinical experience? Experience and Deliberate Practice
What is your “Philosophy of care”? Get as many patients seen as possible? Increase patient volumes by 10%? Insure every patient gets recommended care? Think of the worst thing that could be going on with the patient and rule it out? Save money? Avoid unnecessary radiation and testing? Role of “Philosophy” of your team and facility
Some philosophies may be at odds Increase volume vs. provide safe care If care is barely being safely provided at present volume, how can you expect higher volume will allow safe care without system changes? Trauma service functions with safeguards and double checks for a ICU census of 8—10 and a floor census of 10-12 What happens when ICU census increases to 20 and floor census increases to 25?? Do you have a contingency plan that goes into effect (like the military, police and fire do) Philosophy
Just telling people to “try harder” or “make less mistakes” or “take better care of the patients” rarely is an effective strategy Most people are trying pretty hard and their output is more dependant on the system they are working in, not their effort “Try Harder”
Can teaching medical practitioners traditional clinical reasoning be detrimental? Naturalistic Decision Making Gary Klein Under conditions of uncertainly, time pressure, and high risk (medicine), experts do not use analytical methods. They use fast and “sufficient” strategies In other words they don’t search for the “best” answer, just the first “acceptable” answer Decision Making
Look at patient and data Fit that data into a schema they have seen before Choose a plan based on their previous experience This is why inexperience is devastating War game the plan and its execution in their head (think about it, you really do this) If plan simulates OK, proceed If it doesn’t step back and form another option Repeat as necessary How do experts make decisions?
Diagnosis has been considered medicine’s central task, but is this best? Having a solid diagnosis can make treatment easier, but the lack of a diagnosis does not relieve the necessity to act Thus the central task of medicine may be management, not diagnosis We should not say, “what is the diagnosis?” but “what should we do now?” (Beth Crandall) Centrality of Diagnosis
Rapid assessment of patients initial presenting data (clinical and digital) Rapid intervention of life threatening signs and symptoms Nothing life threatening Narrow to known condition Mentally simulate treatment and evaluation Proceed with plan Follow results Approach
We don’t teach this well How to rapidly evaluate Find most important data points Assess in relation to other inputs Assign priority to actions Initiate actions Reassess and revise You must practice this by running through scenarios over and over again, or seeing patients with similar problems over and over again Situational Tactics
Mental status change Injury Septic conditions Cardiovascular problems Respiratory problems When we look at avoidable death, almost every case fits in one of these categories Common Emergency Problems
ABC’s and Call Help Protect from further injury or deterioration Rapid exam and assessment of current state and contributing factors Form plan Mental war gaming Initiate May be harder than it sounds Follow-up Common Threads in Safely Treating All These Problems
Tests and double checks fall through the cracks 80 hour does not help this Triage attention to severely ill Leaving less sick to fend for themselves Corrective action Practice Have defined algorithms that you stick to Don’t allow people to improvise just because they are busy Its actually the worst time for them to improvise! Busy Nights (or Busy Units/Services)
Can be insidious Need to screen out occult hypoperfusion and you need to jump on persistently acidotic patients quickly In elderly, persistent acidosis = non-survivor In severe head injury, persistent acidosis = skilled nursing facility “The labs must be wrong, ignore them” Sometimes people don’t want to face the fact the patients is heading in the wrong direction Acidosis