Download
1 / 17
190 likes | 932 Vues
The Nephrotic Syndrome The Nephrotic syndrome refers to a clinical complex that includes the following: Massive proteinuria - 3.5 gm or more/day (24hours) Hypoalbuminemia , with plasma albumin levels less than 3 gm/dl Generalized edema – anasarca

E N D
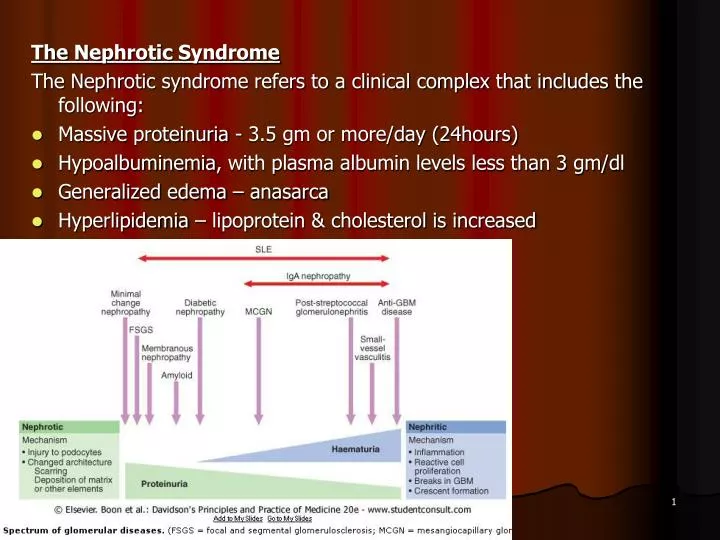
The Nephrotic Syndrome The Nephrotic syndrome refers to a clinical complex that includes the following: • Massive proteinuria - 3.5 gm or more/day (24hours) • Hypoalbuminemia, with plasma albumin levels less than 3 gm/dl • Generalized edema – anasarca • Hyperlipidemia – lipoprotein & cholesterol is increased Dr S Chakradhar
Initially - derangement in the capillary walls - resulting in increased permeability to plasma proteins. • Protein to escape from the plasma into the glomerular filtrate - hypoalbuminemia • Drop in plasma colloid osmotic pressure and primary retention of salt and water by the kidney - generalized edema • Hypoalbuminemia triggers increased synthesis of lipoproteins in the liver and impairment of peripheral breakdown of lipoproteins. • The lipiduria - reflects the increased permeability of the GBM to lipoproteins. Dr S Chakradhar
Common causes: • Minimal lesion GN. • Membranous GN. • Focal Segmental glomerulosclerosis • Membranoproliferative • Mesangiocapillary GN • Chronic pyelonephritis • Diabetes mellitus. • Amyloidosis. • SLE. • Drugs & Infections Dr S Chakradhar
A. In children: • Minimal lesion & Focal lesion are common. B . But in adult: • Membranous lesion is more common than children. C. In adult: i) Diabetes mellitus. ii) Chronic pylonephritis. iii) Amyloidosis • SLE & other systemic causes are common. Approximate prevalence of primary disease = 95% in children, 60% adults. Approximate prevalence of systemic disease = 5% in children and 40% in adults. Dr S Chakradhar
Selectivity of Protein When inflammation in Nephron : 1. Highly selective: Only low molecular wt. 2. Non selective: Large Molecular Wt. Purpose: 1. To detect the Glomerular damage 2. Highly selective proteinuria respond to steroid Dr S Chakradhar
Symptoms: Oedema • Gradual swelling of the whole body is seen, starting from the face & gradually involving the lower parts of the body • Abdominal discomfort &tightness may develop. • Anorexia, Nausea & vomiting may be present Malnutrition • Frequent infection & muscle wasting Infections Hypercoagulability Features of underlying cause • Rash associated with SLE, or the neuropathy associated with DM Dr S Chakradhar
Signs: • Puffiness of Face with baggy eyelids. • Oedema: Pitting in type & present over lower limbs, sacrum • BP usually normal • Evidence of Ascites may be present. • In Lungs : Pleural Effusion Examination should also exclude other causes of gross edema—especially the cardiovascular and hepatic system. Dr S Chakradhar
Heat coagulation Test (bed side test) • Two thirds of a test tube is filled with urine. • The upper third of the tube is heated up to boiling point over a flame. • If white cloud appears, a few drops of 5% acetic acid is added and the tube is reheated. • If the white cloud increases (egg white colour) it indicates the presence of albumin. But if the cloud disappears, indicates the presence of phosphate Dr S Chakradhar
Investigation Blood • TC, DC, ESR, Hb • Blood Urea, Creatinine, Na, k • Total Protein <6gm% • Total Albumin < 3 gm % • Serum Cholesterol: raised Dr S Chakradhar
Investigation Urine (Routine & C/S) • 24 hours urinary total protein : Massive proteinuria - > 3.5 g/ day • Chest X-ray ( to see pleural effusion) • According to secondary cause like DM, SLE, hepatitis etc • Renal Biopsy - Confirmatory Dr S Chakradhar
Differential Diagnosis: • Heart failure • Liver failure: Hepatitis/Cirrhosis of Liver • Acute fluid overload Dr S Chakradhar
General measures 1.Diet : salt restriction (No added salt), Avoidance of High protein diet 2. Control of Oedema: Diuretics- spironolactone or thiazide or frusemide • 40 mg Frusemide at 8 am • 40 mg at 2 pm with k supplement 3. Daily wt. of the pt. to detect progress of oedema 4. To prevent secondary infection give Antibiotics 5. Atrovastatin for hyperlipidemia Dr S Chakradhar
Specific measures 1.Steroid therapy for minimal change nephropathy i)In Children • 60 mg/m2/day in 3 divided doses for 4 weeks followed by • 40 mg/m2/day in a single dose on every alternate day for 4 weeks. ii)In Adults • Prednisolone 1mg /kg/day for 8 weeks then the dose is gradually reduced & stopped in 6 months Dr S Chakradhar
Relapses • Prednisolone 2 mg/kg/day till urine becomes negative for protein. Then, 1.5 mg/kg/day for 4 weeks. Frequent relapses • Cyclophosphamide or cyclosporin 2.Membranous Glomerulonephritis • Treated with corticosteroids & immunosuppressive drugs 3.Treatment of the underlying disease such as SLE 4. Achieving stricter blood glucose control if diabetic. 5.Blood pressure control with ACE inhibitors are the drug of choice. Independent of their blood pressure lowering effect, they have been shown to decrease protein loss. Dr S Chakradhar
Complications: • Hypercoagubility - Venous thrombosis • Hypovolaemia leads to hypovolaemic shock. • Pulmonary edema • Infection – Peritonitis, CRF, RTI • Effects due to steroid – Osteoporosis, Diabetes, PUD, Growth retardation. • Effects due to Cyclophosphamide - Bone marrow depression, Peripheral neuropathy Dr S Chakradhar
Prognosis: • Depends on the cause • Usually good in children, MCD responds very well to steroids and does not cause chronic renal failure. • Other causes such as FSG frequently lead to ESRD • Factors associated with a poorer prognosis - level of proteinuria, BP control and GFR Dr S Chakradhar