Download
1 / 22
220 likes | 418 Vues
Begin with the end in mind…key principles in EHR adoption and use (experiences with open health architecture) . Sarah Chouinard, MD Community Care of WV, CMO and David Campbell, CEO Community Health Network of WV. Community Health Network of West Virginia and PCS/CCWV.

E N D
Begin with the end in mind…key principles in EHR adoption and use (experiences with open health architecture) Sarah Chouinard, MD Community Care of WV, CMO and David Campbell, CEO Community Health Network of WV
Community Health Network of West Virginia and PCS/CCWV • The West Virginia Primary Network, Inc., dba Community Health Network of West Virginia (the “Network”) is the first health-center controlled network in the country to successfully adapt a version of the Resource and Patient Management System (“RPMS”) health information system of Indian Health Service (“IHS”) for use in the community health center setting. • Primary Care System in Clay, WV (now part of Community Care of WV) was the pilot site for adaptation and implementation of RPMS by the Network. Dr. Chouinard served as Chief Medical Advisor and Chairperson of the Clinical Committee that coordinated implementation with Network support staff and contractors.
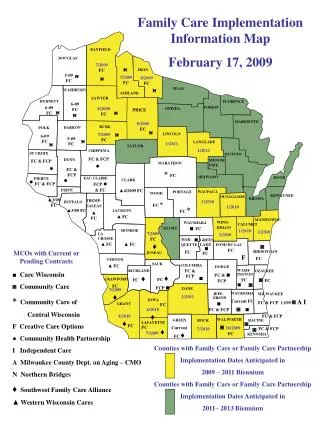
Use of RPMS as a health improvement solution by CHNWV • The deployment of RPMS is part of a multi-faceted approach by CHNWV to aggressively address the chronic conditions facing West Virginia. The Network project is an integral part of the state’s approach to quality improvement through HIT deployment. • The Network staff has trained more than 800 clinicians and administrative support personnel in seven CHC member organizations operating 37 clinical locations; more than 195,000 patient files are included in the Network’s RPMS database (over 10% of West Virginia’s population). • The Network’s health improvement initiative supports member health center efforts to use Care Model and Medical Home concepts to meet the needs of an aging and chronically-ill population and to prepare for the newly developed “meaningful use” HIT criteria.
Open Source Healthcare and West Virginia VistA Public Domain Electronic Medical Record software operated by the Department of Veterans Affairs. Currently deployed in 7 state hospitals and long-term care facilities in West Virginia. RPMS VistA based solution developed by Indian Health Services, for ambulatory care. Operated in 37 clinics within West Virginia. First major installation outside of Indian Health Services facilities by CHNWV.
Selection of RPMS as an HIT solution • The project is based upon a modified version of the Chronic Care Model (the “Care Model”) developed by Ed Wagner, M.D., (Group Health Center for Health Studies) and disseminated by the Institute for Healthcare Improvement. • The Network created a “Clinical Committee” comprised of medical directors and clinical representatives of participating health centers during the evaluation and selection of RPMS as the platform for the system. • The Network Clinical Committee participated in testing of the VistA Office EHR system as part of a pilot program with the Centers for Medicare & Medicaid Services (“CMS”) and members of the Committee also evaluated commercial alternatives.
Outcomes driven health improvement • The Network Clinical Committee, working with Network staff and state officials identified a number of key targeted health improvement areas based upon prevalence and severity of chronic conditions facing most Network member health centers. • These conditions include diabetes, cardiovascular disease, weight management and physical activity, asthma and tobacco use. • The Clinical Committee started with the nationally-recognized outcome measures for these conditions and worked back to the optimum clinical processes necessary to achieve significant improvement in the outcomes. This process served as the roadmap for configuration and implementation of RPMS as a common health improvement tool shared by participating care teams.
Population-based, patient centered health care • The Network Clinical Committee also premised the Network’s health improvement project on the six key components of the Care Model: the community in which the primary care center resides; the health system itself; self-management support; delivery system design; decision support; and clinical information systems. • The intent of this model is to give patients control of their own care, with providers using evidenced-based care practices as members of the patient’s care team. The Committee also incorporated the Six Aims for Improvement of the Institute of Medicine and the concepts of the Medical Home developed by leading professional medical associations. The project has since been adapted to meet “meaningful use” expectations.
Use of RPMS in WV • RPMS was most appropriate system to accomplish project objectives at the time of selection based upon population-based, patient-centered health improvement objectives. • Similar challenges faced by Indian Health Service in managing chronic conditions and RPMS development has been clinically-driven and led; some IHS facilities operate as FQHCs and have same UDS and other reporting requirements. • RPMS is based upon VA’s VistA but has wider range of applications for women, children and ambulatory care. • RPMS is open source (with some proprietary elements) but requires extensive adaptation and configuration for use by CHCs.
Meaningful Use has reshaped the goals of EHR implementation • Prior to Meaningful Use, the goal of EHR implementation was to digitize the traditional office practice. The goal of the EHR was to make seeing patients in the traditional way more efficient by replicating the workflow used in a paper world on the computer. • The traditional approach will no longer suffice to meet the demands of the transformation of care delivery that is happening right now under Meaningful Use and many of the other quality and delivery initiatives (e.g., ACOs, health homes, teaching health centers).
Despite incentives and efforts to drive HIT adoption, we are still in early phase • Increasing but still limited rates of adoption, particularly in small and rural practice settings. • Cost of systems still a barrier to many and there is a digital divide among providers. • Incentives partially offset initial cost but ongoing support is an issue in the absence of reimbursement for use of EHR. • PCAST report notes limitations of current systems and need to enhance data exchange functions – systems will need to evolve over next 3-5 years to meet meaningful use and HIE objectives.
Technology tools should meet clinical objectives – don’t automate an ineffective system of care
Care Teams: who collects what and when and where? • Front Desk Clerk—The Patient Navigator (1) • The Work Up Nurse (1) • The Care Manager (2) • The Check-0ut Clerk (1) • The Outreach Coordinator (1) • The Providers (2) • Ratio for a 2 provider practice 1:1:2:1:1:2 • Ratio for a 6 provider practice 3:2:6:1-2:1-2:6
HIT is a tool for health improvement • One of the lessons learned from the WV experience is that EHRs and HIT are technology tools; process and workflow must be aligned with technology potential to achieve health improvement objectives; • Data must be meaningful to create useful information that drives continuous improvement (garbage in-garbage out); it takes a while to transform data from system into meaningful outcome information; • Care teams must validate data internally to commit to the transformation process and commitment must be continually reaffirmed and celebrated; • Patient engagement is essential and HIT must be integrated into the patient care process to facilitate better self management – next steps – personal health records and health information exchange.
Personal Health Record HealtheMountaineer™ Based on Design from MyHealtheVet. Utilizes federally developed standards for data exchange. Can interpret data from any Meaningful-Use Compliant EHR system (integrated with RPMS as part of demonstration project). Built in open-source technologies. Leverages existing CMS investment thru Medicaid Transformation Grant
Closing Thoughts: • Workflow assessment and realignment is key; • Reorganize your people and use care teams; • Make sure your providers can be efficient and use care managers to coordinate care; • Empower your nurses and patient navigators; • Enable patients (and families) to actively manage health using PHR and portal tools; and • EHR is tool to coordinate health, should support health information exchange and mobile health to take health management to home, workplace and daily living (i.e., interface with assistive technology).