Download
1 / 30
540 likes | 2.4k Vues
TOXOPLASMOSIS. Dr. S.GOPALAKRISHNAN. M.D Asst. Prof. Govt. Hospital for Thoracic Medicine Tambaram. INTRODUCTION. Toxoplasma Gondii is worldwide in distribution. Most common Chronic infection with Obligate intracellular Protozoan in Humans.

E N D
TOXOPLASMOSIS Dr. S.GOPALAKRISHNAN. M.D Asst. Prof. Govt. Hospital for Thoracic Medicine Tambaram.
INTRODUCTION • Toxoplasma Gondii is worldwide in distribution. • Most common Chronic infection with Obligate intracellular Protozoan in Humans. • 3-4 % of all Patients with AIDS may develop CNS Toxoplasmosis at some stage. • Greatest incidence when CD4 < 100 cells/mm3 • Decrease in CMI in chronically infected at risk of reactivation of infection.
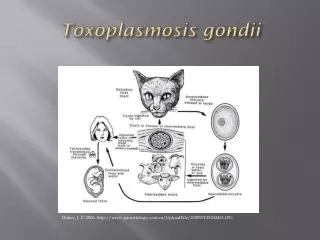
EPIDEMIOLOGY • Definite Host – CAT Sexual Cycle----Oocyst • Intermediate Host– Human,Mouse,Pig,Sheep. Asexual Cycle----Tissue cyst
EPIDEMIOLOGY • Transmission to humans • Oral • Ingestion of under cooked Pork or Lamb meat –tissue cyst. • Exposure to oocysts • Ingestion of contaminated vegetables • direct Contact with cat feces. • Others • Transplacental. • Blood Product Transfusion. • Organ Transplantation.
PATHOGENESIS ORAL INGESTION TACHYZOITE (INVASIVE FORM) DISSEMINATES THROUGH OUT THE BODY INFECTION ->ANY NUCLEATED CELL->MULTIPLICATION -> CELL DESTRUCTION -> NECROTIC FOCI -> SURROUNDING INFLAMMATION TISSUE CYST LIFE LONG CHRONIC INFECTION ONSET OF CMI
SUSCEPTIBILITY – MECHANISM IN HIV • Depletion of CD4 T cells • Decreased production of IL-2 ,IL-12,IFN-g • Decreased cytotoxic T-lymphocyte activity.
CLINICAL PRESENTATION Immuno compromised Cerebral • Manifests primarily as toxoplasmic encephalitis • Altered mental status – 75 % • Focal Neurological deficit – 70 % • Motor weakness • Speech Disturbances • Cranial Nerve Palsy • Movement Disorders • Visual Field Defects • Sensory ,Cerebellar Dysfunction
Cont… • Head ache – 56% • Fever – 45% • Seizures – 30% Extra Cereberal Ocular • Choreoretinitis – Less common than CMV Lesions adjacent to disc, old scar Multi focal, bilateral lesions typically more confluent, thick, opaque. • Anterior Uveitis
Cont… Pulmonary • Highly Lethal sepsis like syndrome • Difficult to distinguish from Pneumocystis cari. pneumonia Cardiac • Asymptomatic • Cardiac tamponade • Biventricular Failure
IMMUNOCOMPETENT • LYMPHADENOPATHY Common – CERVICAL (Single or Multiple non tender,Discrete) Generalized – 20-30% • Fever,Myalgia,Rash , Meningo-Encephalitis. • Rare: Pneumonia,Myocarditis,Polymyositis.
DIAGNOSIS * Serology Anti-IgG Antibodies • Peaks within 1-2 months after infection. • Remain elevated for life. • False negative 10-15% • Sabin-feldman dye test-gold standard • IFA-indirect • Elisa
Cont… • IgM Anti-body tests • Double sandwich Elisa • IFA • Immunosorbent agglutination assay (IgM-ISAGA)
SEROLOGY To diagnose – recent infection • Serial specimens at 3 weeks apart-4 fold increase in IgG titre. OR • Elevated IgM, IgA or IgE titres with differential agglutination test. • Useful to Identify - HIV at risk of developing toxoplasmosis. 97%-100% HIV with toxo –encephalitis have anti IgG anti bodies.
CSF • Non specific • Mild cell count – mononuclear, protein • Intrathecal Anti IgG antibodies production • Ratio > 1 supports the diagnosis of toxoplsmic encephalitis • Wright – Giemsa stain of CSF
DNA • POLYMERASE CHAIN REACTION (PCR) • CSF – Sensitivity 50 – 60% - Specificity 100% • Bronchoalveolar lavage fluid • Vitreous and aqueous humor • Blood samples – low sensitivity: toxo.encpha. • Amniotic fluid • Culture – Time consuming
NEURORADIOLOGIC STUDIES C T • Multiple, bilateral, hypodense, contrast-enhancing focal brain lesions – 70 to 80% • Lesions – basal ganglia, hemispheric corticomedullary junction. • Contrast enhancement often with ringlike pattern
MRI • More sensitive than CT • Identify more lesions than seen on CT, new lesions not seen on CT NEWER IMAGING TECHNIQUES 201T1SPECT: Thallium 201 single- photon emission computed tomography 18F FDG – PET: Fluoride 18 - Flouro – 2 deoxyglucose positron emission tomography.
DEFINITE DIAGNOSIS • Excisional Brain Biopsy: • Usually not performed • Reserved for patients who fail to respond to therapy
DIFFERENTIAL DIAGNOSIS • Primary CNS Lymphoma • Mycobacterial infections • Cryptococcal meningitis • Herpes simplex encephalitis • PML • CMV infection • Infectious mononucleosis
MANAGEMENT IN HIV • Therapy empiric in most cases • Neurologic response • 51% by day 3 • 91% by day 14 • Neuroradiologic study repeated 2-4 weeks after initiation of therapy
Cont… • Acute Therapy • Maintenance Therapy (Secondary Prophylaxis) • Prevention (Primary Prophylaxis) • Discontinuation of Prophylaxis
ACUTE THERAPY • Preferred • Pyrimethamine 200mg po loading dose followed by 75-100 mg po qd plus folinic acid 15-20 mg po qd plus sulfadiazine 1-1.5g po q6h - 6 weeks. • Alternatives • Pyrimethamine with folinic acid (as standard) with one of the following: • Clindamycin 600 mg po q6h • Clarithromycin 1g po bid • Azithromycin 1.2-1.5g po qd • Dapsone 100mg po qd - 6 weeks
MAINTENANCE THERAPY • Preferred • Pyrimethamine 25 mg po qd & folinic acid 10 mg po qd and Sulfadiazine 500-1000 mg po q 6h • Alternative • Pyrimethamine 25 mg po qd & folinic acid 5-10 mg qd po & Clindamycin 300-450 mg po q6-8h. • Atovaquone 750 mg po bid
PREVENTION • To eat well cooked meat - internal temperature of 1160C, or no longer pink inside. • Proper hand washing. • Fruits and vegetables should be washed prior to consumption. • To avoid contact with materials contaminated with cat feces, handling cat litter boxes. • To wear gloves during gardening.
Cont… • Recommended • T gondii - Seropositive patients with CD4 T cell counts <100 regardless of clinical status. • Patients with CD4 T cell counts <200 if an opportunistic infection or malignancy develops. • Trimethorprim / sulfamethazole 1 ds tab po qd • Dapsone 50 m po qd & pyrimethamine 50 mg po q week plus & folinic acid 25 mg po q week
DISCONTINUATION OF PROPHYLAXIS • CD4 T cell counts increase to more than 200 over a period of 3- 6 months in response to HAART • Restarting prophylaxis in patients CD4 T cell counts decrease to < 200