Download
1 / 33
330 likes | 341 Vues
Cathlab hemodynamics – 1 pressures, waveforms ,cardiac output and resistance. Dr .Lakshmi Gopalakrishnan Southern Railway Hospital. HEMODYNAMICS IN CARDIAC CATHETERIZATION. PRESSURE MEASUREMENTS MEASUREMENT OF FLOW VASCULAR RESISTANCE

E N D
Cathlab hemodynamics – 1pressures, waveforms ,cardiac output and resistance Dr .Lakshmi Gopalakrishnan Southern Railway Hospital
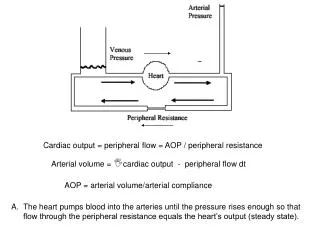
HEMODYNAMICS IN CARDIAC CATHETERIZATION • PRESSURE MEASUREMENTS • MEASUREMENT OF FLOW • VASCULAR RESISTANCE • Principle of Ohm’s Law : Q = ∆ P / R
Pressure recording system • Consists of catheter , transducer, amplifier and recorder • Must meet : • amplitude linearity • adequate frequency response • phase linearity • calibration of transducer over range of amplitudes,and a plot gives linear relationship • optimal damping
Pressure Measurement systems • Fluid filled catheters • Micromanometer catheters
Transducers – to be calibrated against a known pressure, “ zeroed” placing at mid chest level and balanced ( zero all the transducers being used simultaneously) immediately prior to obtaining simultaneous recordings
Fluid filled system - contd Sources of error • Distortion of the output signal due to frequency response and damping charecteristics optimal damping achieved by short, wide-bore , non compliant catheter directly connected to transducer with no air bubbles in the liquid .This achieves frequency response close to output –to-input ratio of 1. • catheter whip artifact, end-pressure artifact, catheter impact artifact, catheter tip obstruction
Pressure measurement – micromanometer system • Advantages include higher natural frequencies, optimal damping characteristics, no whip artifacts • Less distorsion of waveforms, lack the 30- 40 msec delay • Commercially available ones have both end hole and side holes for over the wire use and angiography and ones with two tip transducers for pressure gradients Disadvantages- expense, fragility, added procedure time • Used for research work only.
Normal pressure waveforms Atrial waveforms Right atrium a wave highest Pre – a wave pressure a wave x descent x’ descent v wave y descent Left atrium v wave highest , pressure higher Pulmonary capillary wedge, similar to LA waveform, damped, delayed
Respiratory variation • During spontaneous respiration intrathoracic pressure falls in end expiration by 3-4 mmhg and end-inspiration by 7-8 mmhg • This reduces the RA, LA, Aortic pressures and hence underestimates • All recordings in end expiration since it closely resembles the atmospheric pressure
Atrial waveforms- important points • Shows two positive waves ‘a’ atrial and ‘v’ ventricular and negative waves x’ and y descents • ‘a’ wave is prominent with abnormalities of reduced RV,LV compliance • ‘v’ wave is prominent in AV valve regurgitation • X’ and y descents are diminished in pericardial tamponade • X’ and y descents are accentuated in constriction and restrictive diseases
Ventricular pressure waveform Consists of • Small rapid-filling wave • slow filling wave • ‘a’ wave co-incident with atrial systole • Ventricular systolic pressure wave Pressures reported are early diastolic pressure End- diastolic pressure peak systolic pressure
Arterial pressure waveforms • Rapidly rising systolic pulse wave • ‘ incisura’ • End diastolic pressure • Measured central aortic pressure wave is a conjugate of both forward and reflected waves factors that augment pressure wave reflections vasoconstriction heart failure hypertension ilio femoral obstruction valsalva – after release
Central aortic pressure waveform a conjugate of forward & reflected waves
Aortic pressure waveforms as a function of distance from the Aortic valve
Aortic pressure waveform before & after occlusion of femoral –major increase from augmentation of reflected waves
Cardiac output • Quantity of blood supplied to systemic circulation per unit time in L / min • Determined by preload, heart rate and myocardial contractility • Cardiac index = CO in L / min / m2 BSA • Other variables like age, posture, temperature considered while interpreting CO
Determination of CO - Technique • Fick’s oxygen method • Thermodilution method • Fick’s principle-states that the total uptake or release of any substance by an organ is the product of blood flow to the organ and the art- venous concentration difference of the substance • CO = O2 consumption / AV Oxygen difference • CO = 130 x BSA (Sa O2 – Sv O2) x Hb x 1.36 x 10 • Error in this method -10% Most accurate in low output states and conditions with irregular HR like AF and V bigeminy
Thermodilution method • Injection of 10ml of cold saline in the Right atrium • Measure the temp change in the PA and a transient drop in temp occurs • Curve plotted of the temp of PA vs time • Has a smooth up slope and a more gentle decline • Area under the curve is inversely proportional to the CO CO = CC x (Tb – Ti). Where cc is the computation constant, Tb the blood temperature and Ti the injectate temperature • Severe TR is a contraindication to use of the method Error with this method 5- 20% • Most accurate in high output states and less accurate in low output states
Vascular resistance In clinical practice Ohm’s law : Q = ∆ P / R is used to calculate resistance • Systemic vascular resistance = AO mean - RA mean Q S • Pulmonary vascular resistance = PA mean - LA mean QP pressures are in mmhg , flow in litres per min and resistance in Hybrid resistance unit or Wood’s unit expressed as mmhg / litre/ min • Wood units can be converted to metric units by conversion factor 80 expressed as dynes.sec.cm -5 • Vascular resistance is normalized for BSA giving a Resistance Index. SVRI = Ao(mean) – RA(mean) 80 ______________________ CI Where CI is Cardiac Index. Thus SVRI = SVR x BSA
NORMAL VALUES FOR VASCULAR RESISTANCE Systemic vascular resistance 1170 + 270 dynes – sec – cm -5 Systemic vascular resistance index 2130 + 450 dynes – sec – cm-5 m2 Pulmonary vascular resistance 67 + 30 dynes – sec – cm-5 Pulmonary vascular resistance index 123 + 54 dynes – sec – cm-5 m2