Download
1 / 23
250 likes | 387 Vues
Comparative diagnosis for Toxoplasma gondii in Recurrent Abortive Women Using ELISA ,LAT and PCR.

E N D
Comparative diagnosis for Toxoplasma gondii in Recurrent Abortive Women Using ELISA ,LAT and PCR (1)AL-Thwani, A. N., (2) AL-Saqur,I.M.,and (3) AL-Shemery,B.F (1)Genetics Engendering& Biotechnology for Post graduate Studies, BaghdadUniversity, Baghdad, Iraq (2) Biological Res.Unit for Trop.Dis.,Collage of Science, ,BaghdadUniversity, Baghdad, Iraq (3) Veterinary Collage,
History of the parasite The first known observation of an organism with an appearance like Toxoplasma gondii was made in 1900 by Laveran, who observed the organism in the spleen and bone marrow of Java sparrows. A more definite description was made in 1908 by two French Parasitologists; Nicolle and Manceaux, who found the parasite in the liver and spleen of a North African rodent (Ctenodactylus gondii), The name Toxoplasma was given according to two Greek terms; toxon (arch) and plasma (form
The first definitive observation of T. gondii in humans was made in 1923 by a Czech physician, Janku, who reported the first case of human toxoplasmosis when he observed the parasite cyst in the retina of a child with hydrocephalus and chorioretinitis in a case of congenital toxoplasmosis, but he failed to isolate the organism. Richter (1936) confirmed the role of toxoplasmosis in a case of meningoencephalomyelitis, In IRAQ, the parasite was first recorded by Machattie in 1938 in a smear from spleen and lungs of two stray dogs in Baghdad
Mode of infection Infection occurs during eating the sporulated Oocytefrom infected cat,via food and/ water,unpasteurized milk and its products or the ingestion of bradyzoitein tissue of numerous food animal. Conginetal toxoplasmosisresult from transplacental transmission of the parasites to the fetus causing various degree of damage, dependingon the virulence of the parsite,immune response of the mother and on pregnancy period of the mother ,resulting in featal death or in sever clinical symtomes Primary infection with T. gondii in pregnancy is usually asymptomatic,never the less infection may be transmitted to the fetus causing microcephaly ,retinochorditis and cerebral calcification especially if the woman gets infection for the first time in her life. Infection occurring in thefirst trimesterhave a 10 % chance of transmission to the fetus and have theworst prognosis because the risk of extensive CNS involment,whileinfection occurring in late pregnancyis transmitted to the fetus more frequently, but doesn't cause such extensive damage. Recent report by WHO indicated that 1/3 of world population are infected by this parasite, but the symptom appeared on some of them ( total infection now 500.000 .000
Aims of Current Study Evaluate the diagnostic efficacy for toxoplasmosis by a serologicalmethods (ELISA), (LAT) and molecular method(n PCR) of recurrent aborted women, and their importance in the identification of infection Materials and methods Study Groups' total numbers of 90 aborted and normal women were included in the present study. The study was carried out during the period from December/ 2011 to Feburary / 2012. All patients were obtained from those who had been admitted to / or attended the following health institution in Baghdad: 1. Eben AL-Balady Hospital. 2. Kamal AL-SamaraiHospital.
Blood Samples One sample of 5 ml of venous bloodwas drawn from each subject of this study and was divided into two parts, the first part (3ml) was placed in a sterilized plain tube and left to stand for 30 minutes at room temperature to clot, then centrifuged at 2000 rpm for 10 minutes for serum collection which was aspirated by using micropipette and dispensed into sterile tube and stored in -20°C until used for serological test (ELISA) and (LAT). A second part (2ml) was collected in EDTA tube which used for isolation of genomic DNA from whole blood. Serological Diagnosis 1- Enzyme Linked ImmunosorbantAssay ELISA test determinations were performed with the kits(Toxoplasma-IgM; Toxoplasma-IgG: Biocheck, Inc. Foster City. USA.) and the manufacturer's instructions were followed. 2- Latex Agglutenationtest(LAT) OnSiteToxo IgG/IgM Rapid Test-Cassette (Serum) CTK Biotech, Inc. CA 92121, USA, Catalog Number R0233C was used and the manufacturer's instructions were followed.
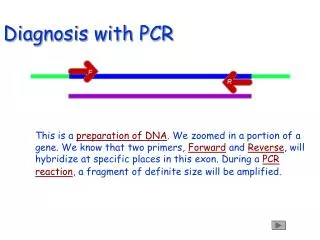
Molecular Diagnosis DNA extraction: DNA was extracted from the whole blood samples using a commercial purification system (Wizard Genomic DNA purification kit, Promega, Madison, WI) following the manufacturer’s instructions. Alternatively, the DNA was rehydrated by incubation the solution overnight at 4○C then DNA was keep in the deep freezer (-20○C) until used. Amplification and Detection of T. gondii DNA by Nested PCR. Nested PCR was performed on all DNA samples to amplify a fragment from B1 gene, which is present in 35 copies and is conserved in the T. gondii genome. The primer used in the first round of the PCR (inner primer pair) are F1(5-GGAACTGCATCCGTTCATGAG-3), and R1(5-TCTTTAAAGCGTTCGTGGTC-3), which correspond to nucleotides 694-714 and 887-868, respectively. The primer used in the second round (outer primer pair) are F2(5-TGCATAGGTTGCAGTCACTG-3)
Results Serological Diagnosis of Toxoplasmosis Detection of anti-T. gondii Antibodies by ELISA The frequency distribution of T.gondii antibodies for patients gave 100% positive result . All control groupgave negative result for T.gondii antibodies
Positive and negative Latex analysis for patients and controls are shown in table. According to such analysis, numbers and percentage frequencies were, 54 (83.1%) of patients samples gave positive results, while 11 (16.9%) showed a negative analysis. In contrast, a control group showed 2 (8%) a positive pattern for toxoplasmosis LAT analysis and 23 (92%) showed a negative analysis. There was a significant difference between patients and control subjects.
Analysis of n PCR results depend on amplification two DNA fragments (193bp and 96bp) of B1 gene in blood sample of infected women figure (1) and (2). The results were exhibited that PCR product of 39(60%) patients' sample showed the band of DNA fragment indicating the presence of B1 gene and that clarified the existence of infection , and 26(40%) showed absence of amplified DNA fragment indicated that no B1 gene and they were free from infection. Molecular method results:-
of control group apparently healthy pregnant women who live with normal style, which showed the band of DNA fragment (positive) and 17(68%) showed absence of amplified DNA fragment (negative). Pearson Chi-square analysis for n PCR results presented significant difference between patients and control subjects
Figure (1): First round of nPCR amplification of (193bp) B1 gene of T. gondii DNA from blood of abortive women and control. Lane-M =marker (100 bp). Lanes 1-4 positive samples. Lanes 5-8 negative samples. Running conditions: Agarose gel (1.5%), 60V. for 2 hrs, stained with ethidium bromide.
Figure (2): Second run of nPCR amplification of (96 bp) of B1 gene of T.gondii DNA from blood of abortive women and control. Lane-M=marker (100bp). Lanes 2-5 are positive samples. Lane 1=negative control. Lanes 6-9 are negative samples. Running conditions: Agarose gel (1.5%), 60V.for 2 hrs, stained with ethidium bromide.
Highly positive results for toxoplasmosis by using serological tests (ELISA technique 65(100%) and Latex test 54(83.1%) compare with positive results of PCR 39 (60%) for the same samples. Such augmentation was dependent on the fact that the diagnosis of toxoplasmosis is made indirectly by serological methods or directly by PCR. The latter dose not depends on an immune response, and allows direct detection of the parasite in biological samples. Thus, they can be used to establish a diagnosis when serological tests are positive.
From the out come of our current study we can RECOMMEND the Followings : • 1-Toxoplamsmosis tests should be conducted before marriage. • 2-Screening the pregnant woman in early month of gestation and those who complete pregnancy for detecting of T.gondii Abs and starting treatment of infected woman and before the transmission of infection to the fetus. • 3-Follow – up of infant born from infected mother.