Download

1 / 54
640 likes | 878 Vues
IN THE NAME OF GOD. Flagship Course on Health Sector Reform and Sustainable Financing; Module 4:. Designing a Health Benefit Package. 2. : Concept & Definition. Kambiz Monazzam M.D July 2005. Definition of Basic package. Defenition of Basic Package of Health Services.

E N D
IN THE NAME OF GOD Flagship Course on Health Sector Reform and Sustainable Financing; Module 4: Designing a Health Benefit Package 2 : Concept & Definition Kambiz Monazzam M.D July 2005
Definition of Basic package
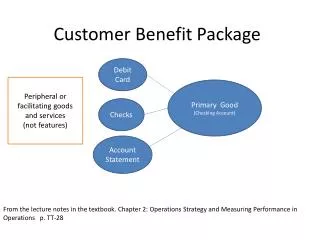
Defenition of Basic Package of Health Services • A limited subset of all health care interventions • Interventions result from a prioritization process • Interventions not independent from each other
Definition: • Basic health package lists health services/goods which are paid by the society because these are deemed to be basic or have priority (Benabbas, 2001).
Common Mistake: • Defining Packages is a decision making process in which we say “ YES ” to a health intervention or say “ NO ” to another one. • Each intervention or a set of interventions need a plan or program of action in which you find all resources, instructions, actions, method of evaluation etc
Limited scope of the basic package: • It cannot include everything • Many services will be omitted • those in the package are the ones value the most.
Prioritization to determine package contents: • Need to criteria that are agreed upon • The agreement can be among policy-makers, the medical profession, or society as a whole • criteria can include, among others, cost- effectiveness of treatments, burden of disease, and/or some combination
Synergistic nature of package interventions: • Individual inputs can complement each other • The whole will be greater than the sum of its parts. In practical terms
Basic Package in Various Contexts
Various Contexts : • Public / Private Mix Provision • Public / Private Insurance Coverage • No availability / entry • Job / Living area / Income (S-E Status) … …
Public vs. private : common situations • Government provision and financing of health services • Guinea, • Private sector provision and financing of health services + Gov. role in provision, financing, and regulation of services • to ensure that efficiency and equity goals can be met
A package is a universal or comparable productwhich helps; • Increases Consumers Choices (health plans, insurers, or different providers) • Simplifies the choices so that they are comparing equivalent products • Important informational and regulatory role • Promote equity
Who Gets the Services in the Package ? • who the package is for, and by extension, who might it not be for? • There are a number of different approaches that can be taken here, all of which may be appropriate in a given country or at a given time. There is no one clear answer here
Approaches to direct package to whom? • Single, Universal Package • Targeted Package for Population Subgroups • Multiple Packages
Single, Universal Package • The package serves as a minimum • The wealthier, will receive at least the same package as the poor, from public resources • Such expenditures could be directed to the neediest and assist in poverty alleviation • Wealthier will be able to get additional services beyond what is offered in the package. • Such an approach creates a two-tier system.
Targeted Package for Population Subgroups • Target the package to specific groups such as poor, pregnant women and children, or those living in particular geographic areas • Equity, Efficiency, Health gains that and access • An example of such an approach is the basic package developed for Bolivia’s Maternal and Child National Insurance Program
Box 2.1 Maternal and Child National Insurance in Bolivia • In June 1996 the Government of Bolivia established the Seguro Nacional de Maternidad y Niñez (Maternal and Child National Insurance-SNMN) as a tool to combat high maternal and child mortality efficiently and equitably. The package is financed from municipality funds earmarked for SNMN on a capitated basis during a first phase, the Government decided to include only a very limited number of interventions in the package. • Maternal Insurance • Prenatal care • Prenatal care for pregnancy with obstetric risk • Care for normal, complicated and cesarean deliveries • Post-partum care • Obstetric emergency care (e.g., third trimester hemorrhaging, pre-eclampsia, premature birth) • Child Insurance • Acute diarrheal diseases • Acute respiratory infections • Neo-natal care • Six months later, following an interim evaluation of the program’s finances and utilization rates, it was determined that there was a financial surplus; the government thus decided to expand the scope of the SNMN basic package by adding another set of priority health interventions for mothers and children. • Source: Escobar, M.L., R. Bitrán and others, 1997.
Multiple Packages • define different packages for different populations or different circumstances • where there are significant geographical variations in costs and disease profiles
Mexico • Mexico’s government proposed three different packages. • One was to expand coverage and provide universal access to essential health services. • Another was for additional cost-effective clinical services that would be available to the working population and their families through a compulsory insurance program. • A third package included all clinical services currently provided through the social security program, but which were too expensive to be financed through the compulsory program. • Progressively “higher” packages thus were directed to smaller and smaller groups, • Sources: Bobadilla, 1996. Harvard University School of Public Health, 1996.
Colombia • Colombia designed a basic package (Plan Obligatorio de Salud-POS) which was to be available to all those participating in the mandatory contributory (i.e., self-financed) program of health insurance. • However, the poor, the unemployed and the under-employed do not participate in this program. Instead they participate in the subsidized program, which is financed with public funds • Sources: Bobadilla, 1996. Harvard University School of Public Health, 1996.
Type of services in Basic package
Types of Services arein the Package? • Public health interventions • Clinical health interventions
Public health interventions • Services that foster changes in personal behavior • Services that control environmental hazards • Services give specific health care to the population
Clinical health interventions • Different levels of facilities may provide different responses to similar health problems • The clinical intervention itself may not be significantly different from one facility to another; However, the resources that may be required may be very different
Preventive vs. Curativeinterventions: • public health and preventive approaches should take precedence (analytical terms) • It is unlikely that public health interventions can be successful in preventing all morbidity; as a result, there will always be a need for some level of clinical interventions. It is important to reach an appropriate balance between the two.
Provision of services
How to Provide the Services • Public-Private Mix in Provision • The Transition
Public-Private Mix in Provision • How efficiency in production can be achieved? • A common assumption is that the private sector works more efficiently than the public sector. This is often true.
The Transition Process • How quickly we can move to that scenario? • Direct demand to private facilities, close down public facilities, and use those resources for other purposes (such as monitoring and regulation). However, this cannot be done due to political and social opposition.
The Transition Process cont, • How quickly we can move to that scenario? • Difficulty of the transition is in the referral system—a package would ideally encourage (or require) people to use primary health care facilities rather than 2-3rd level hospitals. • However, many of these facilities are not currently equipped or staffed to meet the potential demand, part of the reason being that the existing referral system fails.
Financing shifts: • Public hospitals in Colombia traditionally received “supply subsidies” from central government revenue, which were used for their operating expenditures. • Under the new health insurance program, all hospitals (and health facilities) will receive payments based on the services which they provide to a particular population. Thus, there will be a shift to “demand subsidies”—the concept is that the money follows the patient wherever he or she goes.
Determining the Cost of package
Determining the Costs of the Package • What financing available • Different interventions & costs • Determine the marginal cost
Marginal cost • Marginal cost information is often more difficult to obtain than average cost data • Relying on average cost information, which may have no relationship to marginal costs, can greatly under-estimate the actual cost of a package
Exercise: • Child vaccination in a village: 100 children/ one nurse • Personnel 1 nurse $50 per month = $50 • Vaccines 100 units $0.50 per unit = $50 • Suppose we want to immunize one additional child. This target child lives in a neighboring village, • Personnel 1 nurse $50 per month = $50 • Vaccines 101 units $0.50 per unit = $50.50 • Fuel and maintenance = $25
Answer • Total cost: $100 • Average cost of immunizing 101 children: $1.00 • Total cost: $125.50 • Average cost of immunizing 101 children: $1.24 • Marginal cost of immunizing the 101st child $25.50
. • marginal costs will increase as an intervention becomes increasingly available
Type of services in Basic package
How to Finance the Package of Services • Public resources • Private resources
Public resources(1) • Health services with public good characteristics • Providing information to consumers • Promoting equity and ameliorating poverty
Public resources(2) • How to determine what level of public resources should be made available to finance the package?
Private resources(1) • A certain amount of cost-sharing or co-payments could be required, to help cover some of the costs of the package, • Moral Hazard, Where can it be applied; for example, drug costs • Care must be taken that those who are truly needy are exempted from financial requirements
Private resources(2) • Co-payments on a sliding scale basis … • Cross-subsidization • mandated contributions are made in accordance with income (Rising percent) • Do you Suggest it for Iran?
Which one is financially better in terms of equity?& Why? What is your suggestion for the worst one?
Who is Responsible? For making this Important decision Who says Yes? Who says No?
In Iran the health package was defined over ten years ago in two major categories: • First, the preventive services which are provided free. • Second are curative services that are financed by insurance organizations. • There is an exclusion list comprising cosmetic surgery, organ transplantation, infertility and scoliosis.
What’s the problem: • The major problem in adding a new service to the list without prioritizing and allocating extra resources is: • 1- Financial bankruptcy • 2- Low quality services • 3- High out of pocket payments • 4- Greater financial risk to the people (catastrophic health expenditure).
Health Package Responsibility: • The health package is regulated by High Council for Health Insurance (HCHI). • Decision to exclude or include an item is opinion based • Decisions is not evidence based.
Present situation: • Almost all countries have some intrinsic priority setting mechanism, but the current decision-making process in the public sector, which is based on implicit criteria, is unsatisfactory, because of a lack of transparency and distortion in the allocation of resources. • With few exceptions, establishing priorities is not evidence based and is heavily influenced by political pressures (Bobadilla, 1998).