Download
1 / 1
30 likes | 227 Vues
Hospital Care & Transitions. 1. Preliminary Information (Spell all names) a. Patient spelling, MRN, PATCOM b. Dates of Admission/Discharge c. Attending Physician, Service (e.g. ‘Gen Med Team 3’) d. Person Dictating

E N D
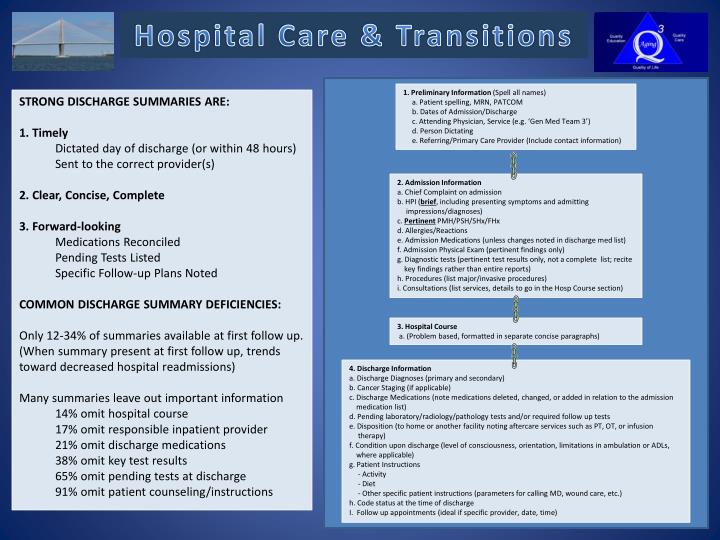
Hospital Care & Transitions 1. Preliminary Information (Spell all names) a. Patient spelling, MRN, PATCOM b. Dates of Admission/Discharge c. Attending Physician, Service (e.g. ‘Gen Med Team 3’) d. Person Dictating e. Referring/Primary Care Provider (Include contact information) • STRONG DISCHARGE SUMMARIES ARE: • 1. Timely • Dictated day of discharge (or within 48 hours) • Sent to the correct provider(s) • 2. Clear, Concise, Complete • 3. Forward-looking • Medications Reconciled • Pending Tests Listed • Specific Follow-up Plans Noted • COMMON DISCHARGE SUMMARY DEFICIENCIES: • Only 12-34% of summaries available at first follow up. (When summary present at first follow up, trends toward decreased hospital readmissions) • Many summaries leave out important information • 14% omit hospital course • 17% omit responsible inpatient provider • 21% omit discharge medications • 38% omit key test results • 65% omit pending tests at discharge • 91% omit patient counseling/instructions • 2. Admission Information • a. Chief Complaint on admission • b. HPI (brief, including presenting symptoms and admitting impressions/diagnoses) • c. Pertinent PMH/PSH/SHx/FHx • d. Allergies/Reactions • e. Admission Medications (unless changes noted in discharge med list) • f. Admission Physical Exam (pertinent findings only) • g. Diagnostic tests (pertinent test results only, not a complete list; recitekey findings rather than entire reports) • h. Procedures (list major/invasive procedures) • i. Consultations (list services, details to go in the Hosp Course section) 3. Hospital Course a. (Problem based, formatted in separate concise paragraphs) • 4. Discharge Information • a. Discharge Diagnoses (primary and secondary) • b. Cancer Staging (if applicable) • c. Discharge Medications (note medications deleted, changed, or added in relation to the admission medication list) • d. Pending laboratory/radiology/pathology tests and/or required follow up tests • e. Disposition (to home or another facility noting aftercare services such as PT, OT, or infusion therapy) • f. Condition upon discharge (level of consciousness, orientation, limitations in ambulation or ADLs, where applicable) • g. Patient Instructions • - Activity • - Diet • - Other specific patient instructions (parameters for calling MD, wound care, etc.) • h. Code status at the time of discharge • I. Follow up appointments (ideal if specific provider, date, time)