Download
1 / 24
240 likes | 373 Vues
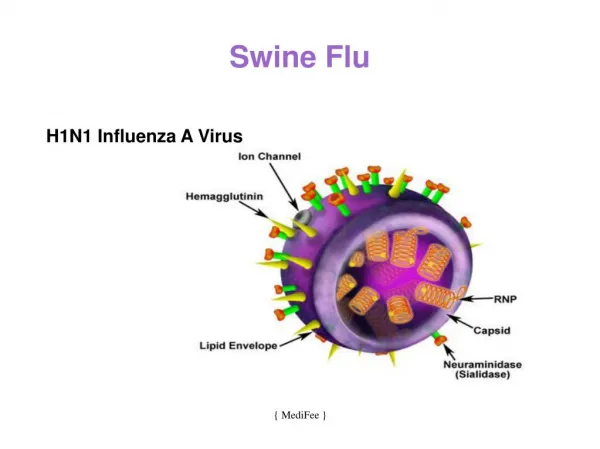
Swine Flu. Preparing for the pandemic 12 th May 2009. Different types of ‘flu. Seasonal influenza Pandemic influenza Avian influenza. The Influenza Virus. Changes in the virus. Antigenic drift - mutation - gradual change Antigenic shift - reassortment of antigens

E N D
Swine Flu Preparing for the pandemic 12th May 2009
Different types of ‘flu • Seasonal influenza • Pandemic influenza • Avian influenza
Changes in the virus • Antigenic drift - mutation - gradual change • Antigenic shift - reassortment of antigens - abrupt change - new sub type
Spread of virus • Person to person • Survives for a short time on surfaces • Incubation period of 18-72 hours • Infectious 24 to 48 hours after onset of symptoms • Children may be infectious for longer
Uncomplicated influenza • Fever (38-40oC) • Headache • Myalgia • Dry cough • Nasal discharge
Pulmonary complications • Croup in young children • Primary influenza virus pneumonia • Secondary bacterial pneumonia • Strep pneumoniae • Staph aureus • Haem influenzae
Non-pulmonary complications • Myositis • Cardiac complications • Encephalopathy Also, Reye’s Syndrome and Guillan Barre
Swine Flu from Mexico Initial reports: • about 60-70 deaths • A few hundred cases Subsequent epidemiology: • Infects about 1 in 3(seasonal flu is 1 in 10) • Slightly higher death rate than seasonal flu • Severity of symptoms and complications? • All deaths outside Mexico in people with co-morbidities
Diagnosis • Nose and throat swabs • Use of PCR but can also grow the virus Suspect/possible case - based on clinical symptoms and one of a) travel or b) contact with a case Probable case - swab has confirmed influenza A (usually in a few hours) Confirmed case - tests confirm H1N1 (takes a few days)
Treatments Neuroaminidase inhibitors • Oseltamivir – Tamiflu • Zanamivir – Relenza • reduce duration of uncomplicated influenza by 1 day in 70-90% of people 2. Limited evidence - may reduce serious complication in high risk • Approved for prophylaxis and treatment 4. How do they work in pandemic situations?
Cases in the UK(as of 11th May 2009) • 65 confirmed cases • 336 people still awaiting results • No deaths • Worldwide – over 5000 cases in 30 countries, and 4 deaths outside Mexico
Approach to containment in UK • No restrictions on travel and mass gatherings • Identification of potential cases • Treatment of cases • Administration of prophylaxis to close contacts • First 3000 cases
Handling in general practice • Managing high anxiety amongst patients/population • Discouraging possible cases from attending health care premises • Swabbing and treating on advice of Health Protection
PCT workstreams (1) Aims: 1. Manage large numbers of people with symptoms 2. Prevent spread to the vulnerable 3. Reduce burden on existing health services
PCT workstreams (2) - Arrangements for assessment of cases under PGD - Distribution of antivirals to patients we assess to patients assessed by GPs to front line health care workers - Use of personal protective equipment getting supplies training in use/fitting - Communicating to MOP
What happens if things get worse? Large numbers of ill people and people with severe illness • General practice may be swamped • Hospitals may be under huge pressure • Significant numbers of health and care service staff may become ill • People may need to take time off to look after children and relatives • Supplies of health related products (eg antibiotics) • General supplies
What have we planned for • Practices have had a template and many have thought about business continuity • A borough influenza pandemic plan to oversee the response • Distribution of antivirals • GP/Community services plan - practices continuing as normal for as long as possible - eventually a single command and control arrangement for practices that cannot continue – use of EMdoc
Practices need to now consider (1) • What is essential care? • Which services need to be prioritised? • Have all practice staff been engaged in thinking about the issues? • Is basic information easily available (eg telephone numbers)? • Resilience around different functions eg if clinical staff are not in, how will others manage.
Practices need to now consider (2) • Roles of individuals, eg practice manager • Supplies for the surgery • Length of prescriptions • Telephone consultations • Can things be done differently • Buddy up with neighbouring practices • Checklist from RCGP
Communications • With practice staff • With hospitals/hospices/mental health trusts • With London Borough of Bromley - carers -schools • With patients and the public!
BBC news – 12th May 09 Professor Niall Ferguson at Imperial: “full pandemic potential” “virus similar to 1957 pandemic” (which caused about 2 million deaths worldwide) “major epidemic in autumn and winter in the Northern Hemisphere”