Download
1 / 50
560 likes | 844 Vues
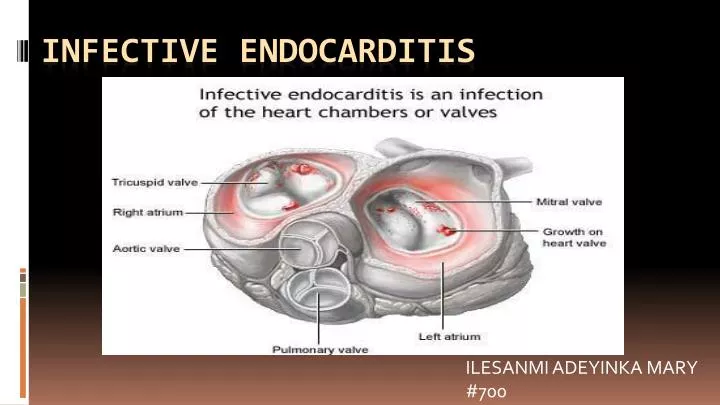
ILESANMI ADEYINKA MARY #700. Infective Endocarditis. Definition :. Infection of the endocardial surface of heart characterized by - Colonization or invasion of the heart valves (native or prosthetic) or the mural endocardium by a microbe,

E N D
ILESANMI ADEYINKA MARY #700 Infective Endocarditis
Definition: • Infection of the endocardialsurface of heart characterized by • - Colonization or invasion of the heart valves (native or prosthetic) or the mural endocardium by a microbe, • - leading to formation of bulky, friable vegetation composed of thrombotic debris and organisms • - often associated with destruction of underlying cardiac tissue.
Sitesinvolved: • Heart valves(commonly) • Mural endocardium • Intracardiac devices • Ventricular septum defects
RISK FACTORS FOR SPECIFIC PATHOGENS THAT CAUSE IE • Dental procedures, poor dental hygiene - viridans streptococci, nutritionally variant streptococci, HACEK • Prosthetic valves – Early: coagulase negative staphylococci, S. aureus – Late: coagulase negative staphylococci, viridans streptococci • Gastrointestinal or genitourinary procedures - enterococci or S. bovis (colon carcinoma) • Nosocomial - S. aureus (including MRSA), Gram negatives, Candida species
CLASSIFICATION : Infective endocarditis may have an indolent, subacute course or a more acute, fulminant course with greater potential for rapid decompensation. • Acute bacterial endocarditis (ABE): • usually develops abruptly and progresses rapidly (i.e, over days). • A source of infection or portal of entry is often evident. • When bacteria are virulent or bacterial exposure is massive, ABE can affect normal valves. • It is usually caused by S. aureus, group Bhemolytic streptococci, pneumococci, or gonococci.
Subacute bacterial endocarditis (SBE): • usually develops insidiously • progresses slowly (i.e, over weeks to months). • Often, no source of infection or portal of entry is evident. • SBE often develops on abnormal valves after asymptomatic bacteremia due to periodontitis, GI, or GU infections. • SBE is caused most commonly by streptococci (especially viridans, microaerophilic, anaerobic, and nonenterococcal group D streptococci and enterococci) and less commonly by S. aureus, Staphylococcus epidermidis, and fastidious Haemophilus sp.
Post oprativeendocarditis or PVE • develops in 2 to 3% of patients within 1 year after valve replacement and in 0.5%/yr thereafter. • It is more common after aortic than after mitral valve replacement and affects mechanical and bioprosthetic valves equally. • Early-onset infections (< 2 mo after surgery) are caused mainly by contamination during surgery with antimicrobial-resistant bacteria (eg, S. epidermidis, diphtheroids, coliform bacilli, Candida sp, Aspergillussp). • Late-onset infections caused mainly by contamination with low-virulence organisms during surgery or by transient asymptomatic bacteremias, most often with streptococci; S. epidermidis; diphtheroids; and the fastidious gram-negative bacilli, Haemophilus sp, Actinobacillus.
Microbiology: • Staphylococcus aureus(35%) : Either healthy or deformed valves, IV drug abusers (polymicrobial), devices • Streptococcus viridans(32%) : Native but previously damaged/abnormal valves • Enterococci (8 %) • Coagulase negative staphylococcus - S. epidermidis (4%): Prosthetic valve endocarditis, devices • Gram –ve bacilli of HACEK group (4%) • Yeast and Fungi(1%)
Pathogenesis: • Portal of entry: • Dental / Surgical Procedures • Contamination by IV drug use • Obvious infections (RS/Skin) • Occult source from gut, oral cavity • Trivial injuries. • Intravascular catheter infection • Nosocomial wounds • Chronic invasive procedures
Morphology: • Friable, bulky and potentially destructive vegetation containing fibrin, inflammatory cells, and microbes. • The vegetations form either systemic or septic emboli • Aortic and mitral valves involved most commonly. • Tricuspid valve involvement in iv drug users.
Symptoms: Acute High grade fever and chills SOB Arthralgias/ myalgias Abdominal pain Pleuritic chest pain Back pain Subacute Low grade fever Anorexia Weight loss Fatigue Arthralgias/ myalgias Abdominal pain
Signs: • Fever • Heart murmur • More specific signs - Osler’s Nodes, Janeway lesions, and Roth Spots • Nonspecific signs – petechiae, “splinter” hemorrhages, clubbing, splenomegaly, neurologic changes
Petechiae • Nonspecific • Often located on palpebral conjunctiva, buccal and palatal mucosa and the extremities
Splinter Hemorrhages • Non-specific • Non-blanching • Linear reddish-brown lesions found under the nail bed • Usually do NOT extend the entire length of the nail • Vessel damage from swelling of the blood vessels (vasculitis) or tiny clots that damage the small capillaries (microemboli).
Osler’s Nodes- immune • More specific • Painful, erythematous and subcutaneous nodules • Located on pulp of fingers and toes • More common in subacute IE
Janeway Lesions • More specific • Erythematous, blanching macules • Nonpainful • Located on palms and soles • Microabscess of the dermis with marked necrosis and inflammatory infiltrate not involving the epidermis.
Roth Spots Oval, retinal hemorrhages with pale centers.
Modified Dukes Criteria for diagnosis of Infective Endocarditis • Definitive Endocarditis if, • - Two major or, • - One major and three minor or, • - five minor • Possible Endocarditis if, • - One major and one minor or, • - Three minor
Major Criteria: • Positive blood culture • Typical organism from two cultures • Persistent positive blood cultures taken > 12 hours apart • Three or more positive cultures taken over more than 1 hour. • Endocardial involvement • Positive echocardiographic findings of vegetations • Myocardial abscess • Development of partial dehiscence of a prosthetic valve • New-onset valvular regurgitation
Minor Criteria: • Predisposition: Predisposing valvular or cardiac abnormality • Intravenous drug misuse • Fever≥38°C (≥100.4°F) • Vascular phenomenon; major arterial emboli, septic pulmonary infarcts, etc • Immunologic phenomenon; glomerulonephritis, osler nodes, etc • Blood cultures suggestive: -organism grown but not achieving major criteria • Suggestive echocardiographic findings
Complications The following are potential complications of IE: • Myocardial infarction, pericarditis, cardiac arrhythmia • Cardiac valvula insufficiency • Congestive heart failure • Aortic root or myocardial abscesses • Arterial emboli, infarcts, mycotic aneurysms • Arthritis, myositis • Glomerulonephritis, acute renal failure • Mesenteric or splenic abscess or infarct
Investigations • Blood cultures: • Key diagnostic investigation in infective endocarditis. • Isolation of microorganism from culture is important for diagnosis and also for treatment. • At least 3 sets of samples should be taken from different venepuncture sites over 24 hours. • Serology: • Can be sent when the diagnosis is suspected and the cultures are negative. • They aid in cases where the organisms will not grow in blood cultures(Coxiella,Legionella,Bartonella)
Chest x-ray • Look for multiple focal infiltrates and calcification of heart valves • EKG • Rarely diagnostic • Look for evidence of ischemia, conduction delay, and arrhythmias • Echocardiography • It can identify the presence and size of vegetations,detectintracardiac complications and assess cardiac function. • Transthoracic echocardiography is noninvasive and has high specificity for visualising vegetations. • Transoesophageal echocardiography is more sensitive than TTE.It can detect small vegetations,prostheticendocarditis and intra cardiac complications.
Complete blood counts may show anemia and increased WBC counts. • Urea and Creatinine: may be elevated due to glomerulonephritis • Inflammatory markers CRP,ESR are increased in infection .CRP also helps in monotoring response to therapy. • Urine proteinuria and hematuria occur frequently.
TREATMENT: Antibotic regimen for infective endocarditis: • Viridians Streptococci and Strep.bovis Penicillin G(12-18g million U IV q24h) continously Gentamicin(3mg/kg 8-12 hourly) 2 weeks Alternative Cefriaxone (2g once daily, iv) 4 weeks Vancomycin (15mg/kg 12 hourly) duration 6weeks
Enterococci • Ampicillin sensitive Ampicillin(12 g IV q24h in 6 divided doses) 4-6 weeks, and Gentamicin(3mg/kg IV or IM q24h in 1 dose for 4-6wk) • Ampicillin resistant Vancomycin+ Gentamicin
. • Staphylococcus aureus • Methicillin-susceptible Nafcillin (12g iv q24h in 4-6 divided doses for 6wk • Both penicillin and methicillin resistant Vancomycin(30mg/kg iv q24h in 2 divided doses for 6wks • Patients with unstable renal function: consider linezoid 600 mg IV q12h
. Surgery: Indications: • Failure of antibiotic therapy • patients with direct extension of infection to myocardial structures. • Prosthetic valve dysfunction. • Congestive heart failure. • Severely damaged valves. • IE caused by fungi or gram-ve or resistant organisms. • Large vegetations on echocardiography • Recurrent embolic attacks. • Abscess formation.
. • Prophylaxis: High risk category: • Prosthetic cardiac valves • Previous bacterial endocarditis,even in absense of heart disease. • Complex cyanotic congenital heart disease (TOF) • Surgically constructed systemic pulmonary shunts. Moderate risk category: • Rheumatic and other valvular dysfunction • Congenital cardiac malformations • Hypertrophic cardiomyopathy • Mitral valve prolapse with valvular regurgitation
Regimen for IE prophylaxis: • Standard oral regime Amoxicillin 2gPO 1hr before procedure • Inability to take oral medication Ampicillin 2g IV or IM 1hr before procedure • Penicillin allergy Clindamycin 600 mg PO Clarithromycin 500 mg PO Cephalexin 2 g PO
CARDIAC MYXOMA
Cardiac Myxoma • WHO defines cardiac myxoma as a neoplasm composed of stellate to plump, cytologically bland mesenchymal cells set in a myxoidstroma • Most common type of primary cardiac tumor (1/3 to ½ of all cases) • Most commonly in 3rd – 6th decade; female > male • Usually solitary and develop in the atria, 75%originating in the left atrium and 15-20% in the right atrium • Arise from or near the interatrial septum at the border of the fossaovalis membrane
Other sites-posterior wall anterior wall appendage • RA myxoma-broader base larger area • Ventricular-free wall/IVS • Multiple- 5% (biatrialcommon).
Etiology • Sporadic vs familial • Majority are sporadic; 90-95% • some are familial which typically arise as part of the CARNEY COMPLEX – a heritable disorder that includes spotty pigmentation of skin and endocrinopathy. PRKAR1A mutation(70%) • LAMB SYNDROME – lentigines, atrialmyxoma and blue nevi • NAME SYNDROME – nevi, atrialmyxoma, myxoidneurofibromas and ephelides
Morphology • Range in size from 1-15 cm in diameter. • Polypoid with a smooth or gently lobulated surface, often pedunculated, and characteristically arise from a narrow stalk. • Polypoid myxomas rarely embolise • Villous or papillary myxomas have multiple fine fragile villous extensions -greatest risk of embolisation.
Histologically-sparsely distributed uniform spindle- and stellate-shaped cells within an extensive myxoidstroma. • Generally hypocellular • stroma and the tumor cells stain positive with PAS, whereas only the stroma shows positive staining with Alcian blue
Clinical presentation • Systemic or cardiovascular findings • Cardiovascular findings: • Atrial • s/sx resemble mitral valve disease most common clinical presentation • Stenosis – tumorprolapse into the mitral orifice during diastole • Regurgitation – injury to the valve by tumor-induced trauma • Ventricular – outflow obstruction syncope
Diagnosis • Two-dimensional transthoracic or trans-esophageal echocardiography • Determine site of tumor attachment and tumor size • Screening of 1st degree relatives for familial or syndrome myxoma • CT scan and MRI • Tumor size, shape, composition, and surface characteristics • Cardiac catheterization • Risk of tumor emboli; for suspected CAD
Myxoma TEE showing a large mass (M), in the left atrium with attachment to interatrial septum and prolapsing through the mitral valve into the left ventricular cavity in diastole. (M = myxoma).
Treatment • Surgical en bloc resection with a margin of normal tissue, if anatomically feasible, is considered curative and is the treatment of choice
Prognosis • Overall risk of recurrence after resection is 13%, but is much more common with familial myxomas (10-20%) than with sporadic tumours (1-3%). • Hazard of recurrence increases linearly for 4 years after resection, after which risk of recurrence is low. • Based on this observation, semi-annual surveillance echocardiographic follow-up has been recommended for 4 years following surgery
Immediate postoperative mortality in most series ranges from 0 to 7.5 percent. • Common postoperative complications include arrhythmias • Recurrence of myxoma in the brain- • Growth of the embolizedtumor fragments, • Difficult to manage, but chemotherapy is not recommended because embolic myxomas do not truly represent meta-static diseases. • Rare but potentially life-threatening complication is the development of cerebral aneurysm secondary to embolic tumor fragments.