Download
1 / 51
560 likes | 921 Vues
Imaging of Thyroid Gland. Bengi Gürses , M.D. Yeditepe University, Medical Faculty Department of Radiology. Anatomy. Located in the anteroinferior part of the neck, outlined by muscle, trachea, esophagus, carotid arteries and jugular veins

E N D
Imaging of Thyroid Gland Bengi Gürses, M.D. Yeditepe University, Medical Faculty Department of Radiology
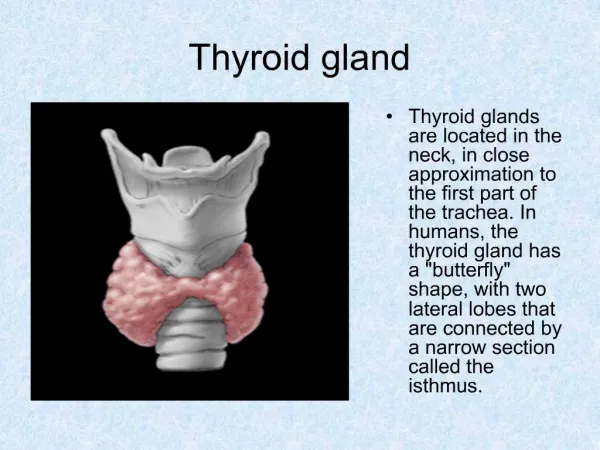
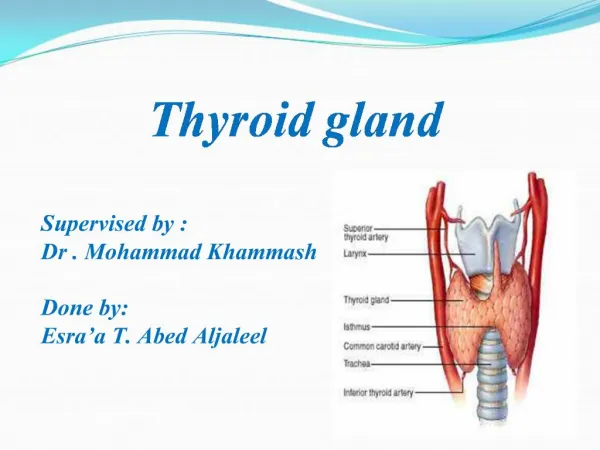
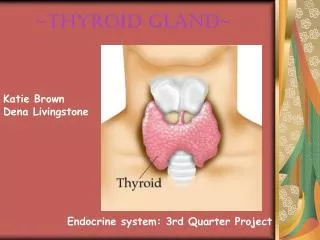
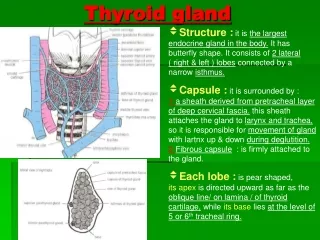
Anatomy • Located in the anteroinferior part of the neck, outlined by muscle, trachea, esophagus, carotid arteries and jugular veins • Two lobes located along either side of the trachea, connected in the midline by the isthmus • Size and shape can vary among individuals • In adults the mean length is 40-60mm, mean AP diameter is 13-18mm. • Mean thickness of the isthmus 4-6 mm
Imaging Modalities • Ultrasound • Computed Tomography • Magnetic Resonance Imaging
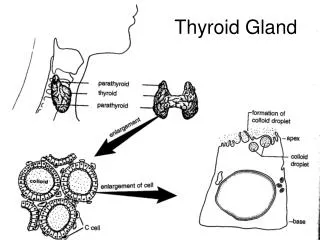
Ultrasound • Primaryradiologicalimagingmodality • US is an accuratemethodtocalculatethyroidvolume • Normal thyroidparenchyma has homogeneousmedium-highlevelechogenicity • IncolorDopplerstudies, thegland is seenhypervascular
Ultrasound • A signalgenerator is combinedwith a transducer. • Piezoelectriccrystals in thesignalgeneratorconvertelectricityintohigh-frequencysoundwaves, whichare sent intotissues. • Thetissuesscatter, reflect, andabsorbthesoundwavestovariousdegrees. • Thesoundwavesthatarereflectedback (echoes) areconvertedintoelectricsignals. • A computeranalyzesthesignalsanddisplaystheinformation on a screen. • Ultrasonography is portable, widelyavailable, andsafe. No radiation is used.
Doppler US • Doppler US is usedtoassessbloodflow. • DopplerultrasonographyusestheDopplereffect (alteration of soundfrequencybyreflectionoff a movingobject). ThemovingobjectsareRBCs in blood. • Directionandvelocity of bloodflow can be determinedbyanalyzingchanges in thefrequency of soundwaves. • Changes in frequency of thereflectedsoundwavesareconvertedintoimagesshowingbloodflowdirectionandvelocity.
Disadvantages • Quality of images depends on the skills of the operator. • Obtaining clear images of the target structures can be technically difficult in overweight patients. • Ultrasonography cannot be used to image through bone or gas, so certain images may be difficult to obtain.
Thyroid Diseases • Congenital Anomalies • Nodular Thyroid Diseases • Diffuse Thyroid Diseases
Congenital Anomalies • Agenesis of one lobe or the whole gland • Hypoplasia • Ectopia (lingual, suprahyoid,pelvic)
Thyroid Diseases • Congenital Anomalies • Nodular Thyroid Diseases • Benign nodule(s) • Malignant nodule(s) Carcinoma Papillary, Follicular, Medullary, Anaplastic • Diffuse Thyroid Diseases
Nodular Thyroid Disease • Thyroid nodule Discrete lesion within the thyroid gland that is sonographically distinguishable from the adjacent parenchyma • Thyroid nodules are very common • Observed at 50% of the population • < 7% of thyroid nodules are malignant • The imaging modality of choice for the investigation of thyroid nodules is US.
Thyroid Malignancy • Papillary Thyroid Carcinoma Excellent prognosis, 20ys 90-95% • Follicular Thyroid Carcinoma Excellent prognosis, 20ys 70% • Medullary Thyroid Carcinoma More aggressive, 10ys 42-90%. May be familial or as a part of MENII syndrome • Anaplastic Thyroid Carcinoma Poor prognosis, 5ys 5%
US Features Suggestive of Malignancy • Suspicious margins, contour and shape • Hypoechoic Solid Nodule • Calcifications • Vascularity • Local invasion and lymph node metastases
Margins, Contour and Shape • Complete uniform halo around a nodule Suggestive of benignity (spec 95%) • Halo / Hypoechoic rim Pseudocapsule of fibrous connective tissue, compressed thyroid parenchyma and chronic inflammatory infiltrates HOWEVER!!! A halo is absent in more than half of all benign nodules 10-24 % of papillary carcinomas have complete / incomplete halo
Margins, Contour and Shape • Ill-defined nodule >50% of the border is not clearly demarcated!! • Suggests malignant infiltration of the parenchyma • No pseudocapsule formation • Sens 7-97% • Some papillary carcinomas may have well-demarcated margin THEREFORE!! Unless frank invasion is demonstrated US appearance of the nodule margins alone is unreliable for determining malignancy or benignity!!
Margins, Contour and Shape • Shape; Not well-described in the literature • Oval shape benign • Solid thyroid nodule taller than wide 93% specificity for malignancy • Thought to be due to centrifugal tendency in growth
Hypoechoic Solid Nodule • Malignant nodules (carcinoma, lymphoma) typically appear solid and hypoechoic • When compared with thyroid parenchyma • Sens 87%, spec 16-27% • Present in also 55% of benign nodules!! • When compared with strap muscles (very hypoechoic) • Sens 12%, spec 94% Marked hypoechogenicity is very suggestive of malignancy!!
Calcification • 2 types • Microcalcification • Coarse calcification • Microcalcification • Specificity for malignancy 85.8% - 95% • Found in 29%-59% of all thyroid carcinomas, most commonly in papillary type. • May be seen in benign conditions such as follicular adenoma, Hashimoto thyroiditis
Calcification • Coarse calcification • Secondary to tissue necrosis • Malignancy rate 75% • Cause posterior acoustic shadowing • Inspissated colloid calcifications cause reverberation artifact Benign!! • Peripheral calcification in MNG >> malignancy
Vascularity • Detected with color / power Doppler US • Intrinsic hypervascularity flow in the central part of the tm greater than the surrounding parenchyma • 69-72% of all thyroid malignancies • However; >50% of hypervascular solid thyroid lesions were benign!! COMPLETELY AVASCULAR NODULE IS UNLIKELY TO BE MALIGNANT!!!
Local invasion and lymph node metastases • Highly specific for thyroid malignancy!! • Clinically; dyspnea, hoarseness, dysphagia • Aggressive local invasion anaplastic thyroid carcinoma, lymphoma, sarcoma.
Local invasion and lymph node metastases • Metastases to regional cervical lymph nodes 19,4% in all thyroid malignancies • Most common in papillary type (40-90%) • Medullary type (50%) • Follicular type – very rare!! • Should be a routine part of US evaluation!!
Metastatic lymph nodes • Rounded bulging shape • Increased size • Replaced fatty hilum • Irregular margins • Heterogeneous echotexture • Vascularity throughout the lymph node (instead of normal central hilar vessels)
Nonspecific US features • Size of nodule • Nodules > 4 cm – more likely to be malignant • Benign nodules may be very large in size!! • Number of nodules • Interval growth of a nodule • Poor indicator of malignancy • The exception; rapid interval growth!!
US Criteria (Benign vs Malignant) Benign Hyper-isoechoic Halo/Hypoechoic rim Peripheric (eggshell) calcification Peripheral vascularity Oval shape LAP Ø Malignant Marked hypoechoic Irregular border /microlobulation Intranodular microcalcification Internal vascularity Taller than wide LAP
FNAB of Incidental Thyroid Nodules • Controversial!! • High prevalence of benign nodules X Low incidence of thyroid carcinoma Low rate of mortality of small thyroid carcinomas • Three sets of guidelines for FNAB (fine-needle aspiration biopsy) of thyroid nodules • Kim criteria • American Association of Clinical Endocrinologists • Society of Radiologists in Ultrasound
FNAB of Incidental Thyroid Nodules • Kim Criteria • A nodule should have at least one of the following findings • Marked hypoechogenicity, irregular or microlobulated margins, microcalcifications, length greater than width. • American Association of Clinical Endocrinologists • A hypoechoic nodule with at least one additional feature should be biopsied • Irregular margins, length greater than width, microcalcifications. • Society of Radiologists in Ultrasound • FNAB should be performed • Microcalcifications within a nodule (>1 cm) • Coarse calcificationwithin a nodule/ Solid nodule (> 1,5 cm) • Mixed cystic and solid nodule (> 2 cm) • Abnormal lymph node • Substantial growth
FNAB of Incidental Thyroid Nodules • In a recent study by Ahn et al. (AJR2010;194:31-37) Kim Criteria and American Association of Clinical Endocrinologists are more accurate!! Kim Criteria higher sensitivity!! AACE higher specificity!!
Thyroid Diseases • Congenital Anomalies • Nodular Thyroid Diseases • Diffuse Thyroid Diseases • Acute suppurative thyroiditis • Subacute granulomatous thyroiditis • Hashimoto’s (chronic lymphocytic) thyroiditis • Painless (silent) thyroiditis • Graves’ disease
Thyroiditis • Acute suppurative thyroiditis Rare inflammatory disease, caused by bacterial infection, usually affects children. On US; frank thyroid abscess. • Subacute granulomatous (DeQuervain) thyroiditis Self-limiting viral disease. Fever, enlargement of gland, pain on palpation. • Hashimoto’s (chronic lymphocytic) thyroiditis Most common type. Autoimmune disease. Young or middle-aged woman. Painless, diffuse enlargement of the gland • Painless (silent) thyroiditis Lymphocytic infiltration in thyroid. Variant form of Hashimoto. No tenderness. May be seen in the postpartum period. • Graves’ disease Extensive lymphocytic infiltration of the gland. Usually characterized by thyrotoxicosis.
US Features in Thyroiditis • Diffuse glandular enlargement • More hypoechoic than normal parenchyma • Coarsened parenchymal echotexture • Multiple discrete hypoechoic micronodules from 1 to 6 mm in diameter (pseudonodular appearance). • Fibrotic septations – pseudolobulated appearance • Vascularity Subacute granulomatous (DeQuervain) thyroiditis • Vascularity Graves’ disease