Download

1 / 11
120 likes | 262 Vues
Cooperation in oral anticoagulant therapy. needs and barriers to improve H. Drewes, M. Lambooij, C. Baan , B. Meijboom, G. Westert. Oral anticoagulant therapy (OAT). OAT reduce the risk of thrombosis Challenge: balance the risk between haemoraghe and thrombosis

E N D
Cooperation in oral anticoagulant therapy needs and barriers to improve H. Drewes, M. Lambooij, C. Baan, B. Meijboom, G. Westert
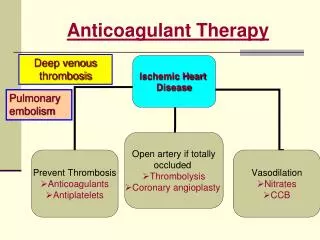
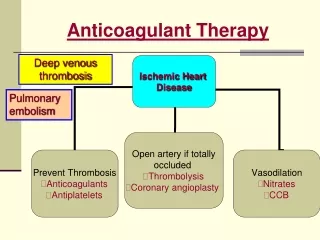
Oral anticoagulant therapy (OAT) OAT reduce the risk of thrombosis • Challenge: balance the risk between haemoraghe and thrombosis • Balance influenced by many factors • e.g. co-medication, fever, food intake, doses advices • Balance influenced by many health care professionals Cooperation needed • No. of patients in NL: 350.000 • 25% of avoidable hospitalizations related to OAT
Anticoagulant clinics (AC) • In Netherlands 59 anticoagulant clinics (ACs): monitoring patients and advice on medication use • ACs provide better patient outcomes than routine medical care However: • Substantial differences in patient outcomes between ACs • Differences in cooperation between ACs • e.g. multidisciplinary protocols, structural meetings etc.
Research questions To identify the bottlenecks for cooperation To identify facilitators/solutions to improve cooperation To identify barriers for improvement the cooperation
Methods • Data • 23 specialised anticoagulant clinics (AC) • selective purposive sampling based on 3 characteristics: • the number of patients • the organisation structure • quality of care considering the patient outcomes • 68 semi-structured interviews
Methods Data analysis • Fully transcriped interviews open coded by two authors • data structured with Chronic Care Model
Experienced bottlenecks • Lack of knowledge: Although a patient was stable with 6 tablets a day, he was discharged with a doses of 4, 2, 2, for the following three days. [..]You could say, ask the patient what he usually used. • Lack of consensus between professionals We don’t agree with the policy of one of our hospitals, but couldn’t convince them. We have to follow their advice; otherwise patients are send home without an operation. • Limited information exchange Really, it is sometime a struggle to get the information about a hospital admission.
Experienced bottlenecks Bottlenecks leads to: - Suboptimal OAT - Inefficacy due to time-consuming effort to correct mistakes
Major Experienced barriers • Lack of motivation • professionals not motivated to learn from ACs (no knowledge) • don’t accept their view (no consensus) • are not motivated to inform the ACs (no information). Lack of time • Lack of resources/ materials
Conclusions • Bottlenecks of coordination are information exchange, lack of knowledge, lack of consensus • Decision support is prerequisite for the succes of AC management as it improves knowledge • Crucial to succesfully implement decision support seems to be informal coordination/contact