Download
1 / 10
100 likes | 105 Vues
“ISSUES FACED BY YOUNG PEOPLE IN SECURE CARE”. Some insights from working in the IVY Project, F-CAMHS, residential children’s homes, secure care, adult NHS settings including forensic mental health services and CAMHS, prisons and legal settings. DR LORRAINE JOHNSTONE

E N D
“ISSUES FACED BY YOUNG PEOPLE IN SECURE CARE” Some insights from working in the IVY Project, F-CAMHS, residential children’s homes, secure care, adult NHS settings including forensic mental health services and CAMHS, prisons and legal settings DR LORRAINE JOHNSTONE Consultant Clinical and Forensic Psychologist Senior Research Fellow Project Lead at IVY Head of Child and Family Clinical Psychology Accredited Assessor for High Courts of Justiciary and DR KATE BLACK Clinical Psychologist at IVY and Creative Psychology in Action
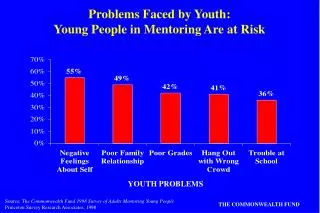
TAKE HOME MESSAGES START AT THE BEGINNING • The parents of children in secure care were, and still are, victims • The medical model prevails: it is a poor fit for this group; we are still responding poorly to parents with PD – despite the serious risk to offspring; • Complex trauma is a lifelong condition and transmitted inter and intra generationally; • Predictable trajectories: traumatised children become LAAC children – then youth justice teenager - then young offenders (70%) and then adult offenders (Forensic Mental Health or Prison). • Early life: little t (e.g. loss, instability, inadequate socialisation, etc.) and Big T (assault, rejection, bullying, lack of autonomy, abuse, neglect)
NEEDS OF YOUNG PEOPLE IN SECURE CARE:WHEN THE OPPORTUNITY HAS BEEN MISSED…
TAKE HOME MESSAGES WHEN THE OPPORTUNITY HAS BEEN MISSED AND THE NEXT ONE ARRIVES…WHAT WE HAVE BEEN DOING • Children are placed in secure care as a last resort – it is an iatrogenic environment – more T and t; • Children in secure care have complex psychological difficulties that may not meet the threshold for CAMHS • Their needs are often too complex and challenging for residential staff to fully address and secure care is not the appropriate setting; • What we know works in secure settings is often not continued when young people leave (high nurture and high structure) • Occasionally CAMHS may seek expert opinions from units down south (often privately funded, high cost and opinion only on whether or not the child meets admission criteria!) or they admit to adult wards locally; • Lack a focus on complex/developmental trauma models
NEEDS OF YOUNG PEOPLE IN SECURE CARE:AN ALTERNATIVE RESOURCE…
15 TAKE HOME MESSAGES AN ALTERNATIVE OR ADDITIONAL RESOURCE MDT interventions are necessary; multi-theoretical psychological formulation is critical to understanding; • At present, IVY is an attempt to fill a void but more needs to be done; • We think, every CAMHS around Scotland should have access to a specialist service for very high risk youth that incorporates assertive outreach and works with all other agencies • IVY is available but not resourced enough to roll-out nationally; IVY provides a narrative account and key treatment goals; • Linked to this, more support required for social workers and Children’s Panel • These children are not the group that are suitable for programmed interventions or manualised treatments (see forensic matrix for guidance). Individualised, multi-model and expertly delivered care plans are necessary with case-study methodology being the more ‘honest’ method of testing Multi-agency Assertive outreach Specialist formulations and interventions Implement Evaluate Idea
TAKE HOME MESSAGES WHEN THE OPPORTUNITY ARISES – WHAT WE SHOULD BE DOING (Perhaps?!) • All children in secure have access to the most expert assessments - MDT interventions are necessary but a psychological/psychosocial assessment, formulation, and intervention is more meaningful; • Children in secure care should have a care plan that incorporates psychological therapies that are assertive, flexible and need and not resource led; • MDT interventions are necessary; multi-theoretical psychological formulation is critical to understanding; • At the moment, both CAMHS and secure care lack a focus on complex/developmental trauma models – these are resource intensive assessments and interventions – both in time and expertise AND • CAMHS often admit to adult wards or transfer down south – we don’t think this is appropriate as a first port of call…there is a serious lack of community resource; • At present, IVY is an attempt to fill a void but more needs to be done; • We think, every CAMHS around Scotland should have access to a specialist service for very high risk youth that incorporates assertive outreach and works with all other agencies – at present, IVY is available but not resourced enough to roll-out nationally; • Linked to this, social workers need to be able to make robust assessments available to the Court to get children placed in stable homes as early possible and Children’s Panel needs to be versed on the impact of parental psychopathology and social problems on childcare; • These children are not the group that are suitable for programmed interventions or manualised treatments (see forensic matrix for guidance). Commissioners of these programmes must be very, very, cautious….for the highest of the high risk group, eclectic, multi-model and expertly delivered care plans are necessary with case-study methodology being the more ‘honest’ method of testing;