Download
1 / 47
490 likes | 1.7k Vues
The Foot Briant W. Smith, MD Orthopedic Surgery TPMG Santa Rosa General Considerations VERY common problems. Systemic disease is a major player (diabetes, vascular and neurologic diseases, inflammatory arthritis) Divide the Foot into Thirds

E N D
The Foot Briant W. Smith, MD Orthopedic Surgery TPMG Santa Rosa
General Considerations • VERY common problems. • Systemic disease is a major player (diabetes, vascular and neurologic diseases, inflammatory arthritis)
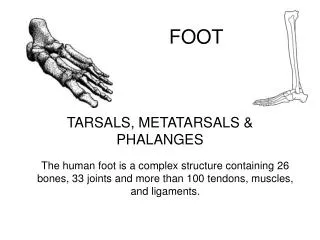
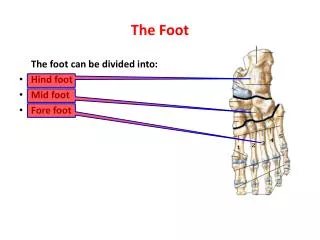
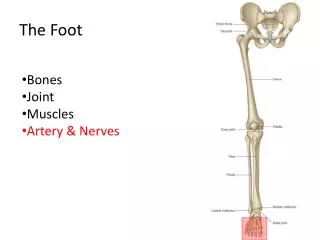
Divide the Foot into Thirds Hindfoot Midfoot Forefoot
Order Standing Radiographs • AP and Lateral are Standing • Oblique is supine
Forefoot Problems • Women far outnumber men because of shoe choices. Shoe modification is the first line of treatment for: • Bunions • Neuromas • Metatarsalgia • Sesamoiditis
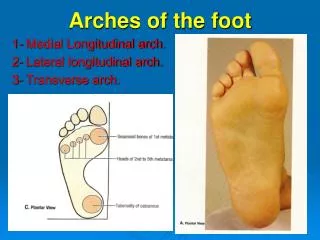
Over-Pronation • Many foot problems are due to excessive pronation (flat feet): • Plantar fasciitis • Achilles and posterior tibial tendinitis • Sesamoiditis • Bunions • Sinus tarsi and tarsal tunnel syndromes • Metatarsalgia
Midfoot Problems Dorsal midfoot pain occurs secondary to arthritis. Bony prominence=‘bossing’ Plantar midfoot pain is rare. Can be plantar fasciitis or fibromatosis.
Hindfoot Problems • Plantar fasciitis is the most common. Pain is plantar/medial. • Heel pad pain is usually a ‘stone bruise’ or due to atrophy of the fat pad. • Posterior tibial tendon dysfunction is the most overlooked problem of the foot.
The Forefoot • Bunions • Funny toes • Metatarsalgia • Interdigital Neuroma • Sesamoiditis • Stress Fracture
BunionsHallux Valgus • The bunion is the enlarged medial prominence of the first MTP joint. • Often there are secondary lesser toe deformities (corns, calluses, hammertoes, bunionette) • Get xrays if patient is going to be referred. • TX: shoe change: widen the toe box, arch + heel support (bunion pads crowd shoe)
1st MTP Arthritis • Hallux rigidus (ortho) or limitus (pod) • 1st MTP can be swollen, spur is dorsal on the xray. • Limited MTP extension (compare to other foot), pain is during the toe-off phase of walking. • Tx with stiff soled shoes, NSAIDs
Funny ToesHammer and Claw Toes • Usually due to IMPROPER SHOE WEAR • Claws are usually seen in diabetics. These are fixed extension of MPJ, and flexion of PIP and DIP joints. • Hammertoes have flexion deformities of the PIP joint, and flexible MP and DIP joints. • Can develop corns and calluses • Tx with wide shoes and toe straps, pads OK; non-operative treatment as long as it is flexible.
It just means forefoot pain. Pain is under a metatarsal head (usually 2nd) as opposed to between the heads for neuromas. Often associated with hammertoes and calluses. Get wider shoes, use metatarsal pads or cut-outs, shave the calluses. Metatarsalgia
Sesamoiditis • Sesamoids are embedded in the flexor hallucis brevis tendon beneath the first metatarsal head. • Caused by repeated stress, and can be inflamed, fracture, or even get arthritic. • Very tender, will move with flex/ext of great toe MPJ. Get xrays. • Tx: stiff shoe, pads/cut-outs; no heels.
Interdigital Neuroma • Really ‘perineural fibrosis’ secondary to repetitive irritation (from tight shoes!) • 90% are in the third interspace; rest in 2nd • Feels like walking on a pebble. Feels better out of shoes. • + squeeze test. Pain is between MT heads. • Tx: wide shoes, MT pads/cut-outs, inject.
Stress Fracture • Pain directly over a metatarsal, usually more proximal than MT heads. • Change in activities, worse with wt bearing • Initial xray often normal. Bone scan positive early. • Tx with modified activity, stiff soled shoe or boot/cast, time.
Midfoot Arthritis • Dorsal bossing or spurs over the involved joint(s). • XR and/or bone scan will show changes. • Tx with stiff soled shoes, firm arch support, NSAIDs, activity modification.
Plantar Fasciits • Pain with arising, especially first AM steps • Almost always at plantar-medial origin. • Inflammation and chronic degeneration. • Worse with obesity, overpronation. • Not due to spurs • Tx: Arch support, elevate heel. NO barefeet, flat shoes; NSAIDs, injections, PT for ultrasound.
Plantar Heel Pain • Can be traumatic (stone bruise) or common in elderly as fat pad atrophies. • Add a pad, like Spenco gel heel cushions.
Posterior Tibial Tendinitis (PTT) • Most missed problem of the foot. • Pain/aching between navicular and medial malleolus. Looks swollen • Flatfeet. Heel should invert with rising on toes. • Tx: arch supports, slight heel. NSAIDs and PT for u/s.
Tarsal Tunnel Syndrome • Post Tib nerve gets entrapped near med malleolus. Plantar tingling/burning as opposed to pain/swelling of PTT. Not whole foot like with diabetes. • + Tinel test; can be loss of PP sensation, can be toe clawing. • Tx: arch support if overpronated. Consider NCV tests.
Foot Examination • Become comfortable with apparent deformities, joint mobility, tendon insertions, vascular and neurologic examinations.
Vascular Examination • Foot color—dependent and on elevation • Edema • Pulses • Capillary Refill • Hair distribution
Neurologic Examination • Lumbar dermatomes vs. specific nerves vs systemic disease • Light touch for gross testing • Semmes-Weinstein 5.07 monofilament for diabetics.
Range of Motion • Should be symmetric • Ankle dorsiflexion 10 deg with knees ext. • Subtalar joint should be mobile. • 1st MTP joint extension should be >60 deg
Tendons • Achilles insertion and body of tendon • Posterior tibial tendon • Peroneal tendons
Deformities • Pump bump • Talar head • NWB and WB for pes planus/cavus • 1st MTP joint • Lesser toes
Treatment Arsenal • Change shoes • OTC arch supports and insoles, pads • Custom Orthotics • Calf stretching/toe rises • Activity modification (swimming/biking) • Weight loss • Night splints/boots/casts
Treatment Options • Physical therapy • Ultrasound • Interferential stimulation • Contrast soaks (10 mins warm, 30 secs ice cold, repeat x2, end with cold) • NSAIDS • Injections