Download
1 / 1

E N D
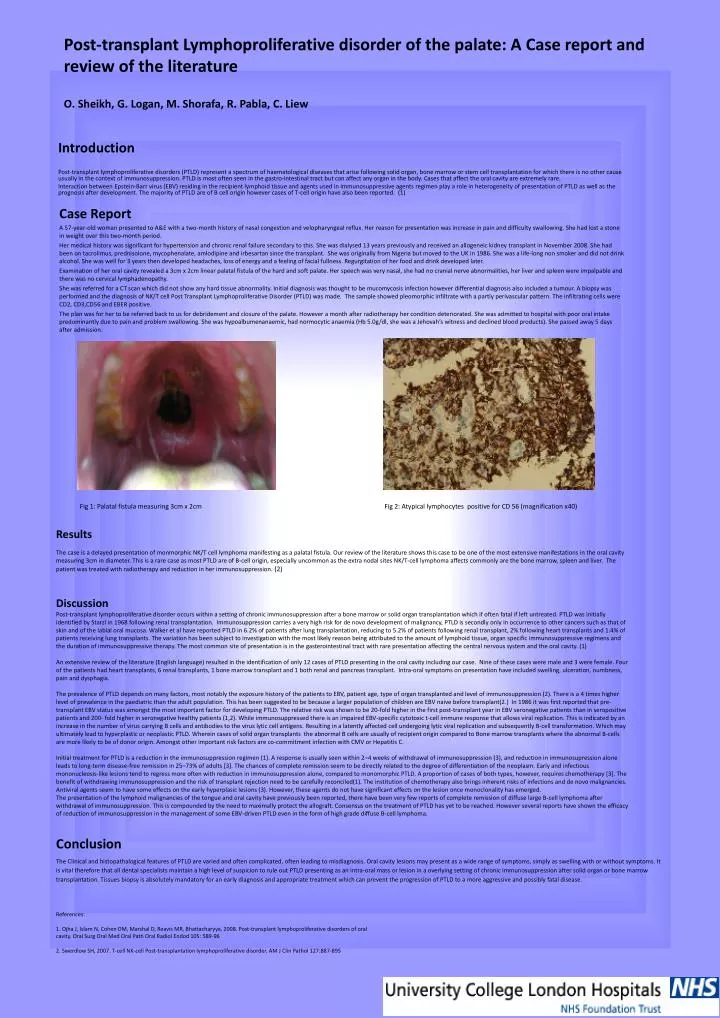
Introduction Post-transplant lymphoproliferative disorders (PTLD) represent a spectrum of haematological diseases that arise following solid organ, bone marrow or stem cell transplantation for which there is no other cause usually in the context of immunosuppression. PTLD is most often seen in the gastro-intestinal tract but can affect any organ in the body. Cases that affect the oral cavity are extremely rare. Interaction between Epstein-Barr virus (EBV) residing in the recipient lymphoid tissue and agents used in immunosuppressive agents regimen play a role in heterogeneity of presentation of PTLD as well as the prognosis after development. The majority of PTLD are of B cell origin however cases of T-cell origin have also been reported. (1) Post-transplant Lymphoproliferative disorder of the palate: A Case report and review of the literatureO. Sheikh, G. Logan, M. Shorafa, R. Pabla, C. Liew Fig 1: Palatal fistula measuring 3cm x 2cm Fig 2: Atypical lymphocytes positive for CD 56 (magnification x40) Results The case is a delayed presentation of monmorphic NK/T cell lymphoma manifesting as a palatal fistula. Our review of the literature shows this case to be one of the most extensive manifestations in the oral cavity measuring 3cm in diameter. This is a rare case as most PTLD are of B-cell origin, especially uncommon as the extra nodal sites NK/T-cell lymphoma affects commonly are the bone marrow, spleen and liver. The patient was treated with radiotherapy and reduction in her immunosuppression. (2) Case Report A 57-year-old woman presented to A&E with a two-month history of nasal congestion and velopharyngeal reflux. Her reason for presentation was increase in pain and difficulty swallowing. She had lost a stone in weight over this two-month period. Her medical history was significant for hypertension and chronic renal failure secondary to this. She was dialysed 13 years previously and received an allogeneic kidney transplant in November 2008. She had been on tacrolimus, prednisolone, mycophenalate, amlodipine and irbesartan since the transplant. She was originally from Nigeria but moved to the UK in 1986. She was a life-long non smoker and did not drink alcohol. She was well for 3 years then developed headaches, loss of energy and a feeling of facial fullness. Regurgitation of her food and drink developed later. Examination of her oral cavity revealed a 3cm x 2cm linear palatal fistula of the hard and soft palate. Her speech was very nasal, she had no cranial nerve abnormalities, her liver and spleen were impalpable and there was no cervical lymphadenopathy. She was referred for a CT scan which did not show any hard tissue abnormality. Initial diagnosis was thought to be mucomycosis infection however differential diagnosis also included a tumour. A biopsy was performed and the diagnosis of NK/T cell Post Transplant Lymphoproliferative Disorder (PTLD) was made. The sample showed pleomorphic infiltrate with a partly perivascular pattern. The infiltrating cells were CD2, CD3,CD56 and EBER positive. The plan was for her to be referred back to us for debridement and closure of the palate. However a month after radiotherapy her condition deteriorated. She was admitted to hospital with poor oral intake predominantly due to pain and problem swallowing. She was hypoalbumenanaemic, had normocytic anaemia (Hb 5.0g/dl, she was a Jehovah’s witness and declined blood products). She passed away 5 days after admission. Discussion Post-transplant lymphoproliferative disorder occurs within a setting of chronic immunosuppression after a bone marrow or solid organ transplantation which if often fatal if left untreated. PTLD was initially identified by Starzl in 1968 following renal transplantation. Immunosuppression carries a very high risk for de novo development of malignancy, PTLD is secondly only in occurrence to other cancers such as that of skin and of the labial oral mucosa. Walker et al have reported PTLD in 6.2% of patients after lung transplantation, reducing to 5.2% of patients following renal transplant, 2% following heart transplants and 1.4% of patients receiving lung transplants. The variation has been subject to investigation with the most likely reason being attributed to the amount of lymphoid tissue, organ specific immunosuppressive regimens and the duration of immunosuppressive therapy. The most common site of presentation is in the gasterointestinal tract with rare presentation affecting the central nervous system and the oral cavity. (1) An extensive review of the literature (English language) resulted in the identification of only 12 cases of PTLD presenting in the oral cavity including our case. Nine of these cases were male and 3 were female. Four of the patients had heart transplants, 6 renal transplants, 1 bone marrow transplant and 1 both renal and pancreas transplant. Intra-oral symptoms on presentation have included swelling, ulceration, numbness, pain and dysphagia. The prevalence of PTLD depends on many factors, most notably the exposure history of the patients to EBV, patient age, type of organ transplanted and level of immunosuppression (2). There is a 4 times higher level of prevalence in the paediatric than the adult population. This has been suggested to be because a larger population of children are EBV naive before transplant(2.) In 1986 it was first reported that pre-transplant EBV status was amongst the most important factor for developing PTLD. The relative risk was shown to be 20-fold higher in the first post-transplant year in EBV seronegative patients than in seropositive patients and 200- fold higher in seronegative healthy patients (1,2). While immunosuppressed there is an impaired EBV-specific cytotoxic t-cell immune response that allows viral replication. This is indicated by an increase in the number of virus carrying B cells and antibodies to the virus lytic cell antigens. Resulting in a latently affected cell undergoing lytic viral replication and subsequently B-cell transformation. Which may ultimately lead to hyperplastic or neoplastic PTLD. Wherein cases of solid organ transplants the abnormal B cells are usually of recipient origin compared to Bone marrow transplants where the abnormal B-cells are more likely to be of donor origin. Amongst other important risk factors are co-commitment infection with CMVor Hepatitis C. Initial treatment for PTLD is a reduction in the immunosuppression regimen (1). A response is usually seen within 2–4 weeks of withdrawal of immunosuppression (3), and reduction in immunosupression alone leads to long-term disease-free remission in 25–73% of adults [3]. The chances of complete remission seem to be directly related to the degree of differentiation of the neoplasm. Early and infectious mononucleosis-like lesions tend to regress more often with reduction in immunosuppression alone, compared to monomorphic PTLD. A proportion of cases of both types, however, requires chemotherapy [3]. The benefit of withdrawing immunosuppression and the risk of transplant rejection need to be carefully reconciled(1). The institution of chemotherapy also brings inherent risks of infections and de novo malignancies. Antiviral agents seem to have some effects on the early hyperplasic lesions (3). However, these agents do not have significant effects on the lesion once monoclonality has emerged. The presentation of the lymphoid malignancies of the tongue and oral cavity have previously been reported, there have been very few reports of complete remission of diffuse large B-cell lymphoma after withdrawal of immunosuppression. This is compounded by the need to maximally protect the allograft. Consensus on the treatment of PTLD has yet to be reached. However several reports have shown the efficacy of reduction of immunosuppression in the management of some EBV-driven PTLD even in the form of high grade diffuse B-cell lymphoma. Conclusion The Clinical and histopathalogical features of PTLD are varied and often complicated, often leading to misdiagnosis. Oral cavity lesions may present as a wide range of symptoms, simply as swelling with or without symptoms. It is vital therefore that all dental specialists maintain a high level of suspicion to rule out PTLD presenting as an intra-oral mass or lesion in a overlying setting of chronic immunosuppression after solid organ or bone marrow transplantation. Tissues biopsy is absolutely mandatory for an early diagnosis and appropriate treatment which can prevent the progression of PTLD to a more aggressive and possibly fatal disease. References: 1. Ojha J, Islam N, Cohen DM, Marshal D, Reavis MR, Bhattacharyya, 2008. Post-transplant lymphoproliferative disorders of oral cavity. Oral Surg Oral Med Oral Path Oral RadiolEndod 105: 589-96 2. Swerdlow SH, 2007. T-cell NK-cell Post-transplantation lymphoproliferative disorder. AM J ClinPathol127:887-895





















