Download
1 / 31
310 likes | 323 Vues
23 Year Old Female of Child Bearing Age with Familial Hypercholesterolemia. Case Categories Primary Prevention Secondary Prevention Pediatric Case Familial Hypertriglyceridemia Diabetes Metabolic Syndrome Low HDL Familial Combined Hyperlipidemia Familial Hypercholesterolemia

E N D
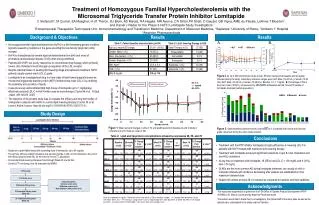
23 Year Old Female of Child Bearing Age with Familial Hypercholesterolemia Case Categories Primary Prevention Secondary Prevention Pediatric Case Familial Hypertriglyceridemia Diabetes Metabolic Syndrome Low HDL Familial Combined Hyperlipidemia Familial Hypercholesterolemia Elevated Lipoprotein (a) Statin Intolerance Case category: Primary Prevention, Familial Hypercholesterolemia, Child Bearing Age History of present illness: 23 year old female of child bearing age with familial hypercholesterolemia. She is interested in advanced testing and treatment recommendations.
Questions to Consider • Question 1 • Question 2 • Question 3 • Question 4
NMR LipoProfile • Insert NMR Lipoprofile 122111 SM88 Insert
Initial Treatment & Management • As she is of child bearing age, start Niaspan 1500 mg/day to lower LDL-P. • Start vitamin D3 5000 IU/day for vitamin D deficiency.
Follow Up on Niaspan 1500 (1 of 2) • Familial Hypercholesterolemia – Improved. • Currently taking Niaspan 1500. • LDL-P lowered from 2111 to 1258. Apo B decreased from 152 to 86. Total cholesterol reduced to 230 from 291. LDL-C dropped from 191 to 111. Non-HDL-C lowered to 135 from 214. Triglycerides are normal at 50. HDL is normal at 77. • Insulin level and free fatty acids are higher at this visit, but may be due to Niaspan. There is no evidence of insulin resistance on NMR. • Sterol testing is abnormal. Will monitor and recheck levels. No need to change treatment, but avoid phytosterol supplements. • Continue therapy. • Elevated CRP – Improved. • CRP lowered from 3.0 to 1.9. • LpPLA2 and MPO remain normal. • Omega 3 index is low at 5.4%. Optimal is >8-10%. • Highest sources of Omega 3 come from Atlantic salmon, herring, mackerel, or Bluefin tuna. • Start Lovaza 1-2 g/day.
Follow Up on Niaspan 1500 • Vitamin D Deficiency – Improved. • Currently taking vitamin D3 5000 IU/day. • Levels increased from 20 to 53. • Continue supplements.
NMR LipoProfile • Insert NMR Lipoprofile 030812 SM88 Insert
Clinical Pearls – Niaspan as Monotherapy • Niaspan is a very effective LDL-P lowering agent. It can be used as monotherapy in women of child bearing age as an agent to lower LDL.
References (1 of 2) Familial Hypercholesterolemia • Cromwell WC, Otvos JD, Keyes MJ, et al. LDL particle number and risk of future cardiovascular disease in the Framingham offspring study – implications for LDL management. J ClinLipidol. 2007 Dec;1(6):583-92. • BrunzellJD, Davidson M, Furberg CD, et al. Lipoprotein management in patients with cardiometabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008 Apr;31(4):811-22. Elevated CRP • National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002 Dec 17;106(25):3143-421. • Ridker PM, Hennekens CH, Buring JE, et al. C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med. 2000 Mar 23;342(12):836-43. APO Genotype • Ballantyne C, Herd JA, Stein E, et al. Apolipoprotein E genotypes and response of plasma lipids and progression-regression of coronary atherosclerosis to lipid-lowering drug therapy. J Am CollCardiol2000;36:1572-8.
References (2 of 2) Vitamin D Deficiency • Dobnig H, Pilz S, Scharnagl H, et al. Independent association of low serum 25-hydroxyvitamin d and 1,25-dihydroxyvitamin d levels with all-cause and cardiovascular mortality. Arch Intern Med. 2008;168(12):1340-1349. • Cannell J, Hollis B, Zasloff M, et al. Diagnosis and treatment of vitamin D deficiency. Pharmacotherapy. 2008;9(1):1-12. • Giovannucci E, Liu Y, Hollis B, Rimm E. 25-hydroxyvitamin d and risk of myocardial infarction in men. Arch Intern Med. 2008;168(11):1174-1180. • Holick M. Vitamin D Deficiency. N Engl J Med. 2007;357:266-81. • Michos E and Blumenthal R. Vitamin D Supplementation and Cardiovascular Disease Risk. Circulation. 2007;115(7):827-828. • Hathcock J, Shao A, Vieth R, et al. Risk assessment for vitamin D. Am J ClinNutr. 2007;85:6-18. • Jockers B. Vitamin D sufficiency: An approach to disease prevention. The American Journal for Nurse Practitioners. 2007;11(10):43-50. • Perez-Castrillon J, Vega G, Abad L, et al. Effects of atorvastatin on vitamin D levels in patients with acute ischemic heart disease. Am J Cardiol. 2007;99(7):903-4.