Download
1 / 35
430 likes | 1.07k Vues
Peritonitis Priorities. Paul Finan Department of Colorectal Surgery Leeds General Infirmary. Peritonitis Classification. Primary - often spontaneous and single organism Secondary - multiple organisms, perforations, leaks, ischaemia etc

E N D
Peritonitis Priorities Paul Finan Department of Colorectal Surgery Leeds General Infirmary
PeritonitisClassification • Primary - often spontaneous and single organism • Secondary - multiple organisms, perforations, leaks, ischaemia etc • Tertiary - no organisms, disturbance in host immune response
Priorities in PeritonitisEarly Recognition • Often classical clinical picture but…. • Beware of immuno-suppressed patients • Elderly patients • Post-operative patients with cardiac problems • Unexplained failure to progress clinically
Peritonitis PrioritiesRadiological Support • Plain films e.g. free gas or unexplained ileus • Abdominal ultrasound – simple collections • CT scanning – of particular value in the post-operative patient • Labelled white cell scans • MR imaging – no experience
Peritonitis Priorities Wound Care Specialists Radiologist Anaesthetist Nutritional Team Nursing Staff Microbiologist Surgical Staff
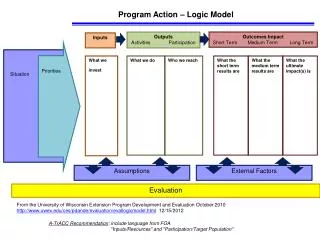
Scoring Systems An effort to quantify case mix and so estimate outcome • APACHE – initially 34 variables • APACHE II – reduced to 12 variables • Sepsis Score (SS) • Sepsis Severity Score (SSS)
Prognostic Scoring Systems in Peritonitis Comparison of APACHE II, APS, SSS, MOF and MPI, in 50 patients with peritonitis • All scoring systems predicted outcome in univariate analysis • APACHE II and MPI contributed independently in a multivariate analysis • All patients with an APACHE II of >20 or MPI >27 died in hospital Bosscha et al 1997
Peritonitis Priorities Source Control Source Control Damage Limitation
Source Control • Drainage of abscesses • Debridement of devitalised tissue • Diversion, repair or excision of focus of infection from a hollow viscus
Source ControlDrainage of abscesses Surgical or non-surgical drainage governed by.. • Clinical state of patient • Site of collection • Extent of collection • Underlying aetiology
Non-surgical Drainage of Intra-abdominal Abscesses A study of PCD in 96 patients with 137 abscesses accumulated over a 3-year period • Successful resolution in 70% after a single procedure and 82% with a second drainage • More often successful in post-operative abscesses. • Poorer results with pancreatic abscesses and those containing yeasts Cinat et al 2002
Non-surgical drainage of Intra-abdominal Abscesses A study of 75 patients undergoing PCD of intra-abdominal abscess • Successful treatment in 62/75 patients (83%) • Success associated with unilocular collections, <200 mls., APACHE score <30 and accessible regions Betsch et al 2002
Source ControlDebridement of Devascularised Tissue • Most commonly encountered in necrotic pancreatitis • Removal of dead bowel • Debridement of other necrotic intra-abdominal tissue
Source ControlManagement of the Source of Contamination • Excision – appendicitis, cholecystitis • Repair – perforated ulcer, early iatrogenic injury • Diversion +/- excision – leaking anastamosis NB These are the decisions that require experience
Damage Limitation • Procedures at the time of surgery • Decisions in the post-operative period
Damage LimitationDecisions at the time of Surgery • Management of the infective source • Peritoneal toilet and removal of particulate matter • Peritoneal lavage • Drains • Wound closure
Damage LimitationPost-operative Decisions • Re-laparotomy • Laparostomy • Interval imaging • Duration of antibiotic therapy
Re-laparotomy in Peritonitis • Failure to progress clinically • Prompted by radiological imaging • Where viability is in doubt • Failure to control source of infection
Relaparotomy for Secondary Peritonitis Meta-analysis comparing planned relaparotomy and laparotomy on demand • No randomised studies • Non-significant reduction in mortality with the latter approach • Evidence based on eight heterogeneous studies Lamme et al 2002
Laparostomy Abdominal wall cannot or should not be closed • Major loss of the abdominal wall • Visceral or retroperitoneal oedema • If decision has already been taken to perform a re-laparotomy • Likelihood of creating abdominalcompartment syndrome
Peritonitis Priorities Wound Care Specialists Radiologist Anaesthetist Nutritional Team Nursing Staff Microbiologist Surgical Staff
Antibiotics in Peritonitis • Consideration to source of infection and likely bacteria • Fewer drugs for shorter periods of time • A policy of reculture and change if necessary • No clear benefit of a particular regimen in the Cochrane review (Wong et al 2005)
Peritonitis PrioritiesConclusions • Multi-disciplinary approach • Increasing role of the radiologist • Emphasis on source control • Need for correct decision at time of laparotomy • Lack of trial evidence