Download
1 / 43

E N D
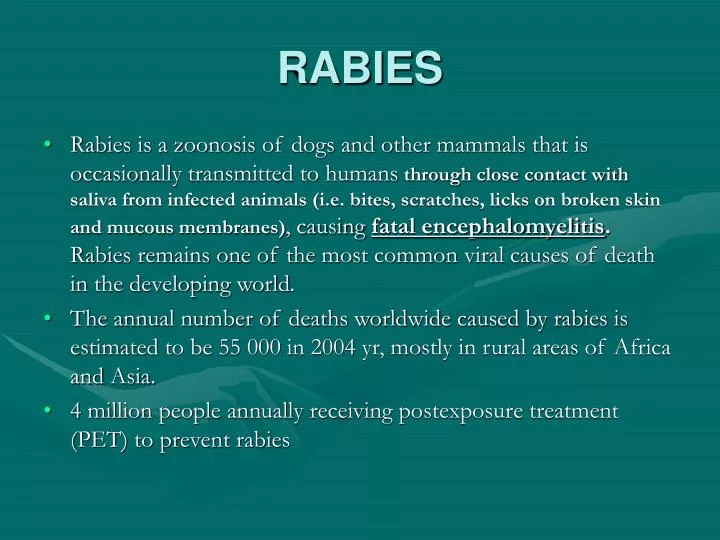
RABIES • Rabies is a zoonosis of dogs and other mammals that is occasionally transmitted to humans through close contact with saliva from infected animals (i.e. bites, scratches, licks on broken skin and mucous membranes), causing fatal encephalomyelitis. Rabies remains one of the most common viral causes of death in the developing world. • The annual number of deaths worldwide caused by rabies is estimated to be 55 000 in 2004 yr, mostly in rural areas of Africa and Asia. • 4 million people annually receiving postexposure treatment (PET) to prevent rabies
Rabies www.travelhealthhelp.com/rabies.html
RABIES • The Greek term for rabies, lyssa, also means "madness" and provides the genus name (Lyssavirus). • Rabies derived from rabare ( to rave). • The Babylon Eshnuna code contains the first known mention of rabies in the 23rd century BC • Rabies virus is a member of the genus Lyssavirus, part of the large family of Rhabdoviruses that infect animals and plants
World distribution of rabies en.wikipedia.org/wiki/Rabies
RABIES • Rabies is currently distributed worldwide except for Antarctica and a few island nations. • Estimates of human rabies mortality rates are notoriously unreliable in tropical areas, where about 99% of the deaths occur. • Areas of high incidence include India, Bangladesh, Pakistan and Nepal, parts of Brazil, Bolivia, Colombia, Ecuador, El Salvador, Guatemala, Mexico, Peru, the Philippines, Sri Lanka, Thailand, and Vietnam
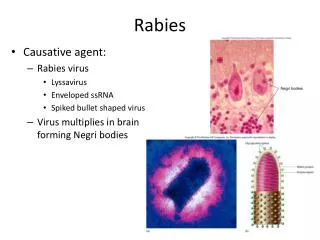
RABIES • Three genera of Rhabdoviridaeinfect animals ( Lyssavirus, Vesiculovirus, Ephenerovirus) • Lyssaviruses comprise seven genotypes, of which rabies is genotype 1, and 6 are rabies-relatedviruses which may also cause fatal human encephalitis • The bullet-shaped virions contain a helical nucleocapsid • The rabies genome is nonsegmented negative strand of rabies RNA encoding five proteins (N, NS, M, G, L).
LyssavirusVirus classification • Group:Group (ssRNA) • Order:Mononegavirales • Family:Rhabdoviridae • Genus:Lyssavirus • SpeciesAravan virusAustralian bat lyssavirusDuvenhage virusEuropean bat lyssavirus 1European bat lyssavirus 2Irkut virusKhujand virusLagos bat virusMokola virusRabies virusWest Caucasian bat virus
RABIES • The epidemiology of human rabies reflects local animal rabies. • In developing areas in which canine rabies remains common, most human cases result from dog bites. In regions where dogs are immunized, most human cases follow exposure to rabid wild animals or bats.
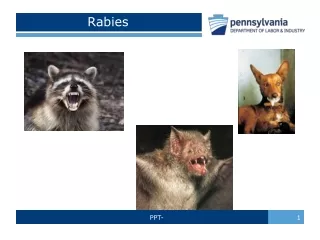
IMPORTANT RABIES VECTOR SPECIES • Africa: domestic dog, jackals • Americas: domestic dog, fox, striped skunk, insectivorous bats • Asia: domestic dog, wolf • Europe: fox, racoon dog, wolf, domestic dog, insectivorous bats,
RABIES- transmission • The virus is usually present in the saliva of a symptomatic rabid animal; • Virus in saliva can penetrate broken skin or intact mucous membranes, and so scratches or licks by a rabid animal may cause infection. • On a few occasions, human rabies has possibly resulted from inhalation of virus in caves that were densely populated by insectivorous bats in the USA, or after laboratory accidents with aerosols of virus. • The saliva, respiratory secretions, and tears of rabies patients contain virus, which could infect another person, • Human-to-human transmission have been documented in recipients of corneal grafts from donors in whom rabies had not been suspected.
RABIES • Rabies virus attaches to acetylcholine receptors at neuromuscular junctions in the bite wound and it is aroute of entry into the nervous system. • During the incubation period- the virus travels to the central nervous system (CNS) by retrograde axonal transport at a rate of 50–100mm/day (in vitro)
Rabies • Rabies infection begins with centripetal spread of the virus via peripheral nerves to the central nervous system (CNS), proliferation within the CNS, and centrifugal spread via peripheral nerve to many tissues
RABIES • Rabies infection requires a period of local viral replication, perhaps to increase the inoculum, before nervous system infection occurs. • Timely administration of antibodies /immunoglobulin/ and active immunization are able to prevent spread of the virus into the nervous system, thereby preventing disease.
RABIES • When the virus reaches the brain, massive replication occurs in neurons by budding from intracellular membranes, and accumulation of viral proteins results in the formation of inclusions (Negri bodies).
Rabies Negri bodies in a neuron www.pathguy.com 30.12.06
RABIES • The high concentration of virus in saliva results from viral shedding from sensory nerve endings in the oral mucosa as well as replication in the salivary glands
RABIES • The virus may persist in macrophages and may later emerge to produce disease. • This may explain some cases with very long incubation periods.
RABIES • Several factors affect the risk and progression of rabies: -the viral inoculum -the location of the bite; bites on the face are more likely to result in disease than those on the extremities. - prominent salivary contamination - multiple bites
Stages of rabies • 1) Incubation period • 2) Prodrome and early symptoms • 3) Acute neurologic disease -furious rabies -paralytic rabies • 4) Coma • 5) Death
RABIES- the incubation period • The incubation period for rabies varies from a few days to more than 19 years, although 75% of patients become ill in the first 90 days after exposure. In 5% patients incubation period is more then 1 year.
RABIES - early symptomps • The prodrome period typically lasts about 4 days. • The initial symptoms of rabies resemble those of other systemic viral infections, including fever, headache, malaise, and disorders of the upper respiratory and gastrointestinal tracts. • Initial neurologic symptoms may include subtle changes in personality and cognition, and paresthesiae or pain near the exposure site. • Myoedema (mounding of part of the muscle struck with a reflex hammer, which then disappears in a few seconds) is present during the prodrome and persists throughout the disease.
RABIES - acute neurologic disease • Human rabies infections are divided into two forms: - furious (or encephalitic) -80% of causes - paralytic (or dumb)-20% of causes
RABIES - the furious form • The furious (hyperactivity) picture of rabies form presents with: -hallucinations, -bizarre behavior, -hydrophobic spasm of swallowing muscles provoked by attempts to drink liquid or by a draught of air on the skin -the hydrophobia, -delirium, -agitation -syndrome of inappropriate antidiuretic hormon
RABIES – the furious form • periodic excitement • aggression, interspersed with lucid intervals, • tachycardia and other arrhythmias, • hypersalivation, • lacrimation, • sweating • fluctuating temperature and blood pressure
Rabies www.en.wikipedia.org www.akolsens.home.att.net
RABIES - the paralytic (dumb) rabies form • is associated with an ascending paralysis, resembling acute inflammatory polyneuropathy (the Guillain-Barre syndrome), or a symmetric quadriparesis. Weakness may be more severe in the extremity where the virus was introduced. - is characterised by lack hydrophobia, aerophobia, hyperactivity, or seizures • meningeal signs (headache, neck stiffness) • paralytic rabies primarily affects the spinal cord, with severe inflammation and necrosis or segmental demyelination
RABIES- coma and death • Acute neurologic syndrome lasts from 2 to 14 days before coma supervenes. • Death occurs an average of 18 days after the onset of symptoms but the range is broad. Intensive support can prolong survival by about 50%.
RABIES • Patients entering coma generally die within 1 to 2 weeks despite maximal supportive care. Furious rabies patients who receive maximal intensive care support and survive for a longer-than-expected period appear to pass into the paralytic phase before death.
RABIES-diagnosis • recognition of an exposure to a potentially rabid animal • viral isolation from saliva, respiratory secretions, CSF, tears, or brain biopsy • virus identification using a panel of monoclonal antibodies (DFA)or by genetic typing- PCR test (during the first week of symptoms, about 50% of samples reveal rabies virus, with an increasing percentage thereafter) • the procedure of choice is DFA analysis of a skin biopsy obtained from the nape of the neck, above the hairline. The virus tends to localize in hair follicles. • detecting neutralizing antibody using (RFFIT), which usually appears 1–2 weeks after the onset of symptoms, and a little later in the cerebrospinal fluid (CSF) • the cerebrospinal fluid (CSF) examination is abnormal in a minority, with a lymphocytic pleocytosis (5 to 30 cells mm3 ), a normal glucose level, and a modest protein level elevation (less than 100 mg/dl). • biopsy or necropsy (animal or human) tissue remains the standard for the diagnosis of rabies
Rabies Diagnosis web.indstate.edu/thcme/micro/CNSvirus/sld009.htm30.12.06
RABIES- differential diagnosis • Encephalitis • Tetanus • Acute inflammatory polyneuropathy, transverse myelitis, or poliomyelitis (paralytic rabies)
RABIES-prophylactic procedures (for domestic animals and selected humans) • Prophylaxis for cats and dogs in many countries is required by law; in the United States, the 3-year vaccines are recommended.
RABIES- preexposure prophylaxis • Preexposure prophylaxis is confined to veterinarians, laboratory workers using rabies virus, and people planning to visit countries of high rabies prevalence • A total of three doses of cell culture vaccine are needed on days 0 and 7 and on day 28 (or day 21) • Booster dosesevery2-3 years prolongs the antibody response
Rabies prophylaxis • Malarial prophylaxis with choloroquine inhibits the antibody response to vaccine given intradermally, so anyone on antimalarial therapy must have intramuscular injections.
RABIES- postexposure prophylaxis • A healthy dog or cat in countries of low prevalence who has bittena human is observed for 10 days. • If the animal's behavior remains normal, the patient need not receive PET beyond proper wound care. If the animal's behavior changes, it should undergo immediate pathologic examination for evidence of rabies infection. • If infection is confirmed, there is adequate time to institute PET. • Wild mammal exposure, especially if theanimal exhibits uncharacteristic behavior, warrants PET in most circumstances. If pathologic examination of the brain does not indicate the presence of rabies virus, PET may be discontinued.
RABIES- postexposure prophylaxis • PET appears safe in pregnant women and should not be withheld when an indication exists.
RABIES-postexposure prophylaxisactive-rabies immune globulin • Post-exposure prophylaxis (P.E.P.) is highly successful in preventing the disease if administered promptly, within 14 days after infection. • The first step is immediately washing the wound with soap and water, which is effective at reducing the number of viral particles. • Rabies immune globulin is available in human and equine forms (pooled antiserum of equine origin and purified antibodies serum of equine origin) Human rabies immune globulin is given in a dose of 20 IU/kg Purified antirabies serum of equine origin is given in a doseof 40 IU/kg
RABIES- postexposure prophylaxispasive-Rabies vaccines • Previous recommendations called for half of the dose to be injected in the vicinity of the wound, and the remainder injected intramuscularly in the deltoid muscle. However, the most recent World Health Organization and Centers for Disease Control and Prevention recommendations call for the entire dose to be infiltrated into the wound if anatomically feasible.
RABIES-postexplosure rabies vaccine schedule • The standard regimen is one dose of tissue culture vaccine (1ml or 0.5ml, depending on the product) intramuscularly on days 0, 3, 7, 14 and 28.
RABIES vaccines • The currently available vaccines for human use in the United States include human diploid cell vaccine (Imovax Rabies), vaccine grown in rhesus monkey diploid cell cultures (rabies vaccine, adsorbed), and purified chick embryo cell vaccine (Rab Avert). • These vaccines are remarkably safe and immunogenic
Rabies- postexposure treatment of previously vaccinated patients • if a neutralizing antibody level has been over 0.5I U/ml at some time, only two doses of intramuscular vaccine are needed on days 0 and 3. • Rabies immune globulin treatment is unnecessary.
RABIES- TREATMENT • There is no established, specific treatment for rabies once symptoms have begun. Despite excellent intensive care, almost all patients succumb to the disease or its complications within a few weeks of onset. • Trials of many agents have been undertaken in clinical rabies, including interferons, interferon-inducing agents, ribavirin, and cytosine arabinoside, without beneficial effects.