Download
1 / 45
450 likes | 709 Vues
Therapy for Follicular Lymphoma. Dr Robert Marcus Kings College Hospital London. Indolent Non-Hodgkin‘s Lymphoma: Overall Survival. 100. 1987-1996 (n=668) 1976-1987 (n=513) 1960-1976 (n=195). 80. 60. %. 40. 20. Horning. Semin Oncol . 1996. 0. s. 0. 5. 10. 15. 20. 25. 30.

E N D
Therapy forFollicular Lymphoma Dr Robert Marcus Kings College Hospital London
Indolent Non-Hodgkin‘s Lymphoma: Overall Survival 100 1987-1996 (n=668) 1976-1987 (n=513) 1960-1976 (n=195) 80 60 % 40 20 Horning. Semin Oncol. 1996 0 s 0 5 10 15 20 25 30 years
Follicular Lymphoma International Prognostic Index (FLIPI) 1.0 0.8 Nodal regions > 4 Elevated LDH Age > 60 Stage III/IV Haemoglobin < 12 g/dl 0.6 Probability of survival 0.4 Good Intermediate 0.2 p < 0.0001 Poor 0 60 72 84 0 0 12 24 36 48 Months Solal-Celigny P, et al. Blood 2004;104:1258–1265.
BNLI Life threatening organ involvement “B” symptoms Bone marrow failure Rapidly progressive disease over any 3–6 month period GELA Bulky disease : nodal/ extranodal mass > 7cm B symptoms Raised B2-microglobulin /LDH Involvement of 3 nodal sites (>3 cm) Splenic enlargement Compression syndrome Pleural/peritoneal effusion Criteria for commencing therapy in FL
“Watch and Wait” versus immediate treatment: overall survival 100 80 60 40 20 0 Cumulative survival (%) Chlorambucil n=158 Observation n=151 0 4 8 12 16 20 24 Time (years) Ardeshna K, et al Lancet 2003;362:516–22
1.0 0.8 0.6 0.4 0.2 0.0 Gene expression-based model of survival following diagnosis of follicular lymphoma Probability p = 9.8 x 10–15 0 5 10 15 20 25 26 Survival (years) Dave SS, et al. N Engl J Med 2004; 351:2159–2169.
Influence of tumour microenvironment on prognosis in FL MARCO scavenger receptor on macrophages SMAD1 transcription factor , mediator of apoptosis and growth arrest EPHA1 tyrosine kinase in transepithelial migration Harjunpää A, et al. Brit J Haematol 2006; 135: 33-42.
The use of prognostic indices • FLIPI is a static measure which relates to populations at risk • Fulfilling criteria for therapy (Watch and Wait) is a dynamic measure which relates to individual patients at a particular point in time • GEP reflects the biology of the tumour or its microenvironment at diagnosis • Can we combine these measures to predict requirement for therapy and decide on which therapy required
In FL more aggressive treatmenthas no impact on survival DFS OS 1.0 0.8 0.6 0.4 0.2 0 1.0 0.8 0.6 0.4 0.2 0 Cyclophosphamide CHOP + bleomycin Cyclophosphamide CHOP + bleomycin Proportion surviving Proportion disease-free 0 2 4 6 8 10 12 14 16 18 0 2 4 6 8 10 12 14 16 18 Years from entry Years from entry Peterson BA, et al. J Clin Oncol 2003;21:5–15
First-line treatment of indolent lymphoma ORR(%) CR(%) Study Treatment n TTP Kimby [1994] Chlorambucil/pred 132 36 5 41%* CHOP 127 60 18 44%* Solal-Celigny [1998] CHVP 119 58 13 18 months CHVP + IFN alfa-2b 123 76 20 34 months (PFS) Hagenbeek [1998] CVP 315 79 45 20 months CVP Þ IFN alfa-2a 120 30 months Hagenbeek [2001] CVP 187 51 15 15 months Fludarabine 194 68 38 21 months Fisher [2000] ProMACE-MOPP 500 83 47 36 months 144 48 months Þ IFN alfa-2a *OS at 5 years
Interferon prolongs survival in FL • Meta-analysis • 10 randomised trials • 1922 patients • If IFN given • with (NOT after) chemotherapydose =/> 5 Mega units • cumulative dose of >36 Mega units/mo • Late survival benefit of 2 years (p=0.0008) 100 80 60 40 20 0 IFN (n=865) Cumulative surviving (%) No IFN (n=1057) p=0.0042 0 2 4 6 8 10 12 Cumulative surviving (%) Rohatiner A, et al. J Clin Oncol. 2005:23;2215–23
AutoPBSCT in 1st Remission FL After : Hiddemann ,W. Brit J Haem 2006
Therapy in the pre-antibody era • No proven benefit for first line: • anthracyclines • PBSCT • Possible benefit for: • interferon with anthracyclines
Rituximab as initial therapyin untreated patients with FL (n=36) PFS same as chlorambucilor nothing!! 1.0 0.8 0.6 0.4 0.2 0 36 patients ORR 72% Progression-free survival 0 1 2 3 4 Years Witzig T, et al. J Clin Oncol. 2005;23:1103–8
Rituximab Post-Induction Regimens (Hainsworth, Ghielmini) * For follicular patients median not reached yet Hainsworth J et al. J Clin Oncol. 2002;20:4261-4267. Ghielmini M et al. Blood. 2004;103:4416-4423.
Intergroup randomised “Watch and Wait” trial in asymptomatic FL Watch and Wait FL Asymptomatic Non bulk No critical organ failure Rituximab 4 weeks standard course Randomisation Rituximab 4 weeks standard course followed by maintenance 1 dose every 2 months for 2 years
New SAKK 35/03 Study Design Short maintenance R Rituximab 375mg/m² every 2 months x 4 Rituximab 375 mg/m² weekly x 4 PR,CR Rituximab 375mg/m² every 2 months until relapse PD, SD off study Long maintenance
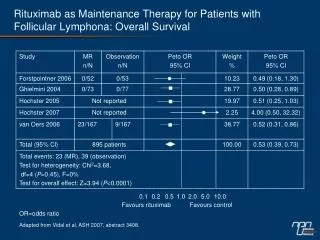
R-CVP versus CVP study design R A N D O M I S E • Follicular NHL (IWF B, C, D) • Stage III−IV • 18 years • No prior Rx • Measurable disease • Central histology review R E S T A G E R-CVP x 4 cycles (q3wk) R-CVP x 4 cycles (q3wk) CR, PR CVP x 4 cycles (q3wk) CVP x 4 cycles (q3wk) SD PD off-study Rituximab 375 mg/m2 iv day 1 Cyclophosphamide 750 mg/m2 iv day 1 Vincristine 1.4 mg/m2 iv day 1 Prednisone 40 mg/m2 po days 1–5 Marcus R, et al Blood 2005; 105:1417–1423.
1.0 0.8 0.6 Event free probability 0.4 0.2 0 0 6 12 18 24 30 36 42 48 54 60 66 72 Time (months) Rituximab-based induction therapy significantly improves time to progression Median follow up of 53 months R-CVP: Median 34 months CVP: Median 15 months p < 0.0001 Marcus R, et al. Blood 2006; 108:Abstract 481.
TTP is significantly improved with R-CVP in all FLIPI subgroups 1.0 1.0 R-CVP CVP 0.8 0.8 Median NR 0.6 0.6 Event-free probability Event-free probability Median 37 months 0.4 0.4 Median 22 months 0.2 0.2 Median 26 months Median 17 months Median 11 months 0 0 0 12 24 36 48 60 72 0 12 24 36 48 60 72 Time (months) Time (months) FLIPI 0–1: Good prognosis p = 0.0288FLIPI 2: Intermediate prognosis p < 0.0001FLIPI 3–5: Poor prognosis p = 0.0009 Marcus R, et al. Blood 2006; 108:Abstract 481.
First-line rituximab-based induction therapy improves overall survival 1. Foussard C, et al. J Clin Oncol 2006; 24:Abstract 7508. 2. Herold M, et al.JCO 2007; April 9 (Epub). 3. Hiddemann W, et al. Blood 2005; 106:3725–3732.4. Marcus R, et al. Blood 2006; 108:Abstract 481.
0 1 22 43 64 85 106 0 1 29 57 85 113 141 CHOP day 1 22 43 64 85 106 B = Bendamustine 90 mg/qm day 1+2 29+30 57+58 85+86 113+114 141+142 R = Rituximab Rituximab 375 mg/qm day 0 29 57 85 113 141 375 mg/qm day 0 22 43 64 85 106 Bendamustine - Rituximab vs CHOP -R B B-R B-R B-R B-R B-R R Tag Randomization CHOP plus Rituximab (CHOP-R) CHOP CHOP-R CHOP-R CHOP-R CHOP-R CHOP-R R Rummel et al ASH 2007 Tag
Progression free survival B-R vs CHOP-R Median observation period 18 months 1.0 p = 0,11 0.9 0.8 0.7 0.6 B-R Probability 0.5 0.4 CHOP-R 0.3 0.2 0.1 0.0 0 12 24 36 48 months
Overall survival improvement with rituximab in FL 1.0 GLSG study NHL 2000 0.8 0.6 GLSG study NHL 1996 Survival probability 0.4 0.2 p < 0.0001 0.0 0 12 24 36 48 60 72 84 96 108 120 Time (months) Number of patients at risk: NHL 1996 538 485 457 419 386 332 242 125 46 0 NHL 2000 794 621 440 250 108 8 0 Hiddemann W, et al. Blood 2006; 108:Abstract 483.
Rituximab maintenance after CVP in untreated indolent NHL: ECOG 1496 study design • Phase III trial of CVP ± rituximab maintenance • 401 patients with previously untreated indolent NHL, 322 randomised R A N D O M I S E D • Rituximab maintenance • 375 mg/m2 q1wk 4 • q6mo 4 CVP 6–8 cycles PR, CR or SD Observation CVP = cyclophosphamide, vincristine, prednisolone.
Rituximab maintenance therapy improves outcomes following first-line induction • ECOG 1496 Phase III study of the 237 patients with FL • 6–8 cycles of CVP induction • Rituximab maintenance therapy* for 2 years versus observation * 375 mg/m2 weekly x 4 every 6 months. Hochster H, et al. Blood 2005; 106:Abstract 349.
R PRIMA Study : Final Design Maintenance (SAKK) 1 dose every 8 weeks for 24 months CR/PR Indolent NHL stages III–IV, untreated CHEMO x 6-8 R x 8 Observation PDs/SDs off study
131I Tositumomab IgG2a antibody labelled with I-131 (gamma emitter ) Murine radio-labelled antibodies in NHL B cell CD20 antigen Tositumomab I 131I Tositumomab B cell 90Y Ibritumomab Ab conjugated via linker to 90Y (beta emitter) CD20 antigen Ibritumomab Tiuxetan 90Y 90Y Ibritumomab
Intergroup European first line follicular lymphoma phase 3 study ? Effect of Rituximab on PFS Start of Study 90Y Ibritumomab Newly diagnosed follicular NHL Stage III–IV Remission induction Chemotherapy** CR /PR No further treatment NR PD Off study **Left to the discretion of the treating physician, e.g. CLB,CHOP,CVP,Fludara etc. **n=400 (accrual complete Jan 2005)
FIT Primary End Point: Median PFS in All Patients* P < 0.0001 Zevalin: median 37 mon = 208 Control: median 13.5 mon = 206 *Median observation period was 3.5 years.
Where next in first line therapy for FL? • UK NCRI trial over 65s : R-CVP vs R-FC + R maintenance • UK NCRI Trial < 65 FLIP 0-2 : i) R-CVP vs R-CHOP ii) Z vs R maintenance • UK NCRI proposed study <65 FLIP 3-5 : R-CHOP – Z vs AutoPBSCT • ? Role for Bendamustine first line
Rituximab maintenance in relapsed/resistant follicular non-Hodgkin’s lymphoma R A N D O M I S E R A N D O M I S E Observation (re-treatment as necessary) CHOP every21 days(maximum 6 cycles) CRPR R-CHOP every21 days(maximum 6 cycles) Rituximab maintenance (375 mg/m2 every 3 months until relapse or for a maximum of 2 years) Van Oers MHJ, et al. Blood 2006 (July 27); ePub ahead of print
PFS after CHOP (n=145) PFS after R-CHOP (n=189) 100 90 80 70 60 50 40 30 20 10 0 100 90 80 70 60 50 40 30 20 10 0 Maintenance Median PFS: 51.8 months Maintenance Median PFS: 42.2 months Progression-free survival (%) Observation Median PFS: 23.0 months Progression-free survival (%) Observation Median PFS: 11.6 months Overall log-rank test: p=0.0043 HR 0.54 Overall log-rank test: p<0.0001 HR 0.30 0 1 2 3 4 5 0 1 2 3 4 5 Years Years Rituximab maintenance significantly improved PFS after response to both CHOP and R-CHOP Van Oers MHJ, et al. Blood 2006 (July 27); ePub ahead of print
RITZ Trial R-Chemo PR, CR R Ibritumomab Rituximab maintenance Rituximab maintenance
Where next in relapsed FL ? • Mini-allo vs auto : a prospective RCT • GA101 – fully humanised anti-CD20 + CHOP/Bend/FCM • Other Moabs : CD80 ( Galiximab)