Download
1 / 45
450 likes | 663 Vues
Cushing’s, Addison’s and Acromegaly. Dr Edward Hutchison FY1 (Geriatrics). Phase II Objectives. 3.21: Investigations – Request appropriately the more common tests of thyroid, adrenal and pituitary gland function, seeking advice where necessary. 3.23: Adrenal gland hormones

E N D
Cushing’s, Addison’s and Acromegaly Dr Edward Hutchison FY1 (Geriatrics)
Phase II Objectives • 3.21: Investigations– • Request appropriately the more common tests of thyroid, adrenal and pituitary gland function, seeking advice where necessary. • 3.23: Adrenal gland hormones • Recognise signs and symptoms of Addison’s disease, confirm diagnosis and initiate immediate management of Addisonian crisis. • Recognise symptoms and signs of Cushing’s syndrome, confirm diagnosis, participat in management of Addison’s disease and Cushing’s syndrome. • 3.24: Pituitary gland hormones • Recognise the circumstances when hypopituiarism might occur, recognise possibility of hypopituitism with ‘non-specific’ symptoms, investigate causes. • Initiate investigation for posterior pituitary function in patients with polyuria. • Recognise acromegaly, initiate investigation for acromegaly, outline to patients the possible treatments for acromegaly.
Aims • HPA Axis • Adrenal glands • Cushing’s syndrome/disease • Addison’s • Acromegaly
Hypothalamus GnRH GHRH TRH Dopamine CRH
Pituitary Sphenoid sinus
Adrenal Glands Remember: GFR!
Functions of Cortisol? • Insulin resistance/gluconeogenesis • Protein catabolism • Immunosuppresion • CVS regulation – e.g. increasing BP • CNS actions – e.g. increased appetite, impaired memory • Increased bone turnover • Gastric acid secretion • Reduced skin collagen • Fluid retention
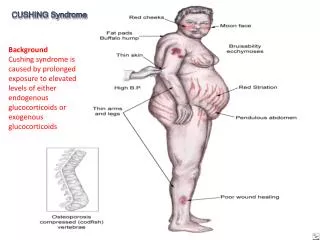
Cushing’s… …disease or syndrome?
Which is which? Syndrome Disease Excessive activation of glucocorticoid receptors. Excessive production of ACTH caused by a pituitary adenoma.
Clinical features Over to you…
Symptoms • Depression • Confusion • Weight gain • Poor glucose control (diabetics) • Weakness rising from a chair (proximal myopathy)
Investigation Bedside Blood Imaging
Not excluded Abstinence ?EtOH excess
Management Untreated Cushing’s disease has a 50% 5 year mortality
Remember • Not only oral corticosteroids can cause Cushing’s syndrome, large amounts of topical and inhaled steroid may be absorbed into the systemic circulation. • Patients on large amounts of oral corticosteroids will require their dose to be tapered slowly to avoid an Addisonian-like crisis. • You also will need to manage the effect of long-term steroid therapy – e.g. diabetes, hypertension, thin skin, osteporosis.
Addison’s disease (Or adrenal insufficiency, to be more correct).
Definition? A syndrome resulting from inadequate secretion of corticosteroid hormones from progressive destruction of the adrenal cortex.
Causes A D D I SO N – autoimmune (90% of cases) – neoplasia (metastases) – degenerative (amyloid) – drugs (e.g. ketoconazole) – infective (TB, HIV) – secondary (ACTH, hypopituitism) – other (e.g. adrenal bleeding)
Clinical Features Over to you…
The short synacthen test • Why do we do it? • How do we do it? • What result do we see in a positive test? (Ruling out Addison’s)
250µg synacthen IM Positive test (ruling out Addisons): Plasma cortisol >460nmol/L at 30 minutes Serum cortisol at 0 minutes Serum cortisol at 30 minutes
Management • Glucocorticoid replacement • Hydrocortisone BD, usually 15mg on waking/5mg around 1800hrs • Excessive weight gain = over replacement • Educate patient – increase hydrocortisone when unwell • Mineralocorticoid replacement • Fludrocortisone 50-100µg daily • Titrate according to symptoms and U&Es
Addisonian Crisis • Features: • Severe shock – hypotension, tachycardia • Fever, abdominal pain, nausea & vomiting • Hyponatraemia/hyperkalaemia ±hypercalcaemia, hypoglycaemia • Management: • ABCDE assessment • Correct volume depletion • Replace glucocorticoids • Correct metabolic abnormalities • Treat underlying cause
Definition? • A condition caused by excessive secretion of growth hormone
Most common cause? • Pituitary macroadenoma
Impress your examiner… Hypopituitism
Management • Conservative: • Patient education • Medical (second line): • Somatostatin analogues (octreotide, lanreotide) • Dopamine agonists • GH receptor antagonists (pegvisomant) • Surgery (first line): • Trans-sphenoidal surgical debulking of pituitary adenoma • Radiotherapy: • Employed if acromegaly persists after surgery
References • Walker, BR., Colledge, NR., Ralston, SH., “Davidson’s Principles of Clinical Medicine” 21st edition, Churchill Livingstone, (2010). • Kumar, P., Clarke, M. “Clinical Medicine” 7th edition, Saunders, 2009. • Longmore, M. et al “Oxford Handbook of Clinical Medicine” 8th edition, Oxford University Press, 2010. • http://www.fipapatients.org/pictures/big/pituitary_normal.jpg • http://www.autismpedia.org/wiki/images/b/b9/Adrenal-core.gif • http://www.ghorayeb.com/files/Transsphenoid_Lateral_380x332.jpg • http://www.nosleeplessnights.com/wp-content/uploads/2013/03/dexamethasone.jpg • http://classconnection.s3.amazonaws.com/319/flashcards/1117319/jpg/addisons_disease1332524676283.jpg • http://upload.wikimedia.org/wikipedia/commons/2/2e/Addisons_hyperpigmentation.jpg • http://globalvoicesonline.org/wp-content/uploads/2012/05/syringe-drawing-320x300.jpg • https://lh5.googleusercontent.com/-qF8wwWfCtFI/TXRv47Ax4xI/AAAAAAAABR8/4jsTaDOngtc/s1600/Synacthen.JPG • http://www.gloshospitals.org.uk/SharePoint11/Pathology%20Web%20Images/Specimen%20containers/Gold_top_with_cap.jpg • http://www.sehha.com/diseases/endocrine/Addison12.gif • http://www.hdwallpapersinn.com/wp-content/uploads/2012/09/bigshow-img.jpg • http://www.examiner.com/images/blog/wysiwyg/image/andre-the-giant.jpg • http://upload.wikimedia.org/wikipedia/commons/1/15/Bitempvf.png • http://www.s2c8.co.uk/wp-content/uploads/2013/01/man-boob.jpg • http://www.physio-pedia.com/images/6/61/Moon_facies_in_Cushings.jpg • http://www.passpaces.com/images/acromegaly_MRCP.jpg