Download
1 / 24
250 likes | 277 Vues
3100A Ventilator. 3100A Ventilator. Approved in 1991 for Neonatal Application for the treatment of all forms of respiratory failure. Approved in 1995 for Pediatric Application, with no upper “weight limit”. For treating selected patients failing conventional ventilation. Theory of Operation.

E N D
3100A Ventilator • Approved in 1991 for Neonatal Application for the treatment of all forms of respiratory failure. • Approved in 1995 for Pediatric Application, with no upper “weight limit”. For treating selected patients failing conventional ventilation.
Theory of Operation • Oxygenation is primarily controlled by the Mean Airway Pressure (Paw) and the FiO2 • Ventilation is primarily determined by the stroke volume (Delta-P) and the frequency of the ventilator.
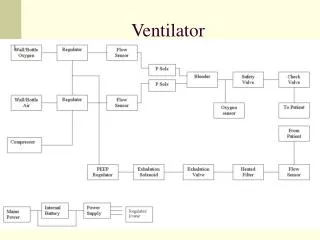
SensorMedics 3100A • Electrically powered, electronically controlled piston-diaphragm oscillator • Paw of 3 - 45 cmH2O • Pressure Amplitude from 8 - 110 cmH2O • Frequency of 3 - 15 Hz • Inspiratory Time • 30% - 50% • Flow rates from • 0 - 40 LPM
Paw is created by a continuous bias flow of gas past the resistance (inflation) of the balloon on the mean airway pressure control valve.
Principle of the SM 3100A HFOV “Super-CPAP” system to maintain lung volume
Oxygenation • The Paw is used to inflate the lung and optimize the alveolar surface area for gas exchange. • Paw = Lung Volume
Optimizing Hemodynamics • PVR is increased with: • Atelectasis • Loss of support for extra-alveolar vessels • Over expansion • Compression of alveolar capillary bed • The lung must be recruited, but guard against over expanding.
Primary control of CO2 is by the stroke volume produced by the Power Setting.
Alveolar ventilation during CMV is defined as F x Vt Alveolar Ventilation during HFV is defined as F x Vt 2 Therefore, changes in volume delivery (as a function of Delta-P, Freq., or % Insp. Time) have the most significant affect on CO2 elimination
Pressure transmission Gerstmann D.
proximal trachea alveoli Pressure transmission HFOV P T
Regulation of stroke volume • The stroke volume will increase if • The amplitude increases (higher delta P) • The frequency decreases (longer cycle time) Stroke volume
The % Inspiratory Time controls the time for piston displacement, controlling CO2 elimination. • Increasing % Inspiratory Time will also affect lung recruitment by increasing delivered Paw.
Inspiratory / Expiratory Ratio • I/E Ratio adjustable with Inspiratory time control • Inspiratory time = Forward movement piston • Expiratory time = Backward movement piston • Backward movement piston = active exhalation ! • Recommended Insp. time = 33% • (prevents air-trapping) + 30% -- 70% Inspiratory time adjustable: 30% - 50%