Download
1 / 36
360 likes | 547 Vues
Current Paradigms in Psychopathology and Therapy. Past and Present Tomàs, J . What is a paradigm?. What do you think???. A Paradigm:. is a conceptual framework to examine a given phenomenon. has a set of basic assumptions .

E N D
Current Paradigms in Psychopathology and Therapy Past and Present Tomàs, J.
What is a paradigm? • What do you think???
A Paradigm: • is a conceptual framework to examine a given phenomenon. • has a set of basic assumptions. Determines which methods (data collection, analysis) will be used to study a given phenomenon.
Paradigms in Abnormal Psychology • Biological • Psychodynamic (Psychoanalytical) • Behavioral • Cognitive • Humanistic
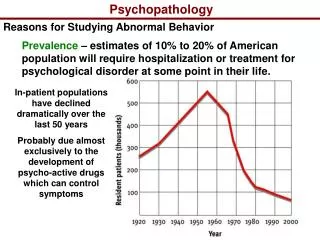
A. Biological Paradigm: Disease Model • Basic assumptions: • 1. Biology plays a role in pathological behavior. • 2. Psychopathology is caused by disease.
What are the flaws with this paradigm? • What do you think???
Flaws with Biological model • 1. Factors unrelated to biology may influence the onset of psychopathology. E.g., environmental factors (life-style, abuse) may play role in some mental disorders (depression). • 2. Multiple factors may influence onset of psychopathology.
Does biology play role in etiology of psychopathology? • What do you think????
Evidence that biology plays a role comes from 2 sources: • 1. Behavioral Genetics – examines how much of individual differences in behavior are due to genetic makeup. • 2. Biochemistry in the nervous system
Behavioral Genetics: Theory • Genotype – the physiological genetic constitution of a person. (fixed at birth, but not static) • Phenotype- the observable expression of our genes (changes over time & is product of interaction with genotype & environment). • E.g., A child may be hard-wired for high intellectual achievement, but will need environmental stimulation to produce development.
We may have a biological predisposition for a mental disorder. • This is called a Diathesis. • Does having a diathesis automatically mean you will develop the mental disorder?
No!!!! • It will depend on how your biology interacts with environmental factors (parental rearing, peers)
How do we study behavior genetics? • 1. Family members • 2. Twin studies • 3. Adoption studies • 4. Linkage analysis
Family Members: • Studies the 1st & 2nd degree relatives of individual with a given mental disorder. • 1st-degree relatives-parents & siblings (50%-shared genes) • 2nd-degree relatives-aunts, uncles (25%-shared genes) • Are compared with index cases (probands).
If there is a genetic predisposition: • 1st degree relatives of the index case(s), should have the disorder at a higher rate than in the general pop. • E.g., 10% of 1st degree relatives of index cases with schizophrenia can be diagnosed with schizophrenia
Twin method • Monozygotic (100% shared genes) & dizygotic twins (50% shared genes) are compared. • Start with diagnosis of one twin & see if other twin develops same disorder. • When twins are similarly diagnosed, they are said to be concordant.
If disorder is heritable-- concordance rate will be higher for MZ than for DZ twins. • Problems: • 1. May reflect environmental factors.
Adoption studies • Examine children who were adopted & reared apart from their “abnormal” parents. • Reduces environmental influences, should reflect effect of genetics.
Linkage Analysis: • Uses DNA blood testing to examine the influence of genetics inmental disorders.
B. Psychodynamic Paradigm: • Argues that our behavior results from unconscious conflicts. • Conflicts are outside of our awareness (iceberg theory).
Structures of mind: • 1. Id (unconscious) “wants” to satisfy basic urges (thirst, hunger, sex). • 2. Ego (primarily conscious) tries to satisfy id impulses without breaking societal norms. • 3. Super-ego (conscious) our morality center which tells us right from wrong.
Psychosexual stages of development • 1. Oral (birth to 1 yr)- needs gratified orally (sucking). 2. Anal (2yr)-needs met- through elimination of waste. • 3. Phallic (3-5 yrs)-needs met through genital stimulation. • 4. Latency (6-12 yrs)-impulses dormant. • 5. Genital (13+)-needs met through intercourse.
Defense mechanisms- unconscious & protect ego from anxiety. • Repression • Projection • Reaction formation • Displacement • Denial • rationalization
Problems: • 1. Freud had no scientific data to support his theories. • 2. Freud’s theories (unconscious, libido, etc.) cannot be observed. • 3. Theory explains behavior (post-hoc) after the fact. • 4. Observations not representative of population.
Freud’s therapy • Premise—we have repressed information in unconscious that needs to come out. • How??? • Free-association, dream analysis, hypnosis.
C. Behavior paradigm • Focuses on observable behaviors. • Premise—abnormal behavior is learned!! • Learning (classical & operant conditioning, modeling)
Classical conditioning • Pavlov’s study: • Step 1: Meat Powder (UCS)---Salivation (UCR) • Step 2: Bell (CS) ---- Salivation (UCR) • -Meat Powder (UCS)---- • Step 3: Bell (CS)---------Salivation (CR)
Conditioning emotional responses: Watson & Raynor • Classically conditioned 11-month-old infant to fear white rats (Santa beard, cotton). • Presented infant with cute white rat—child showed interest in rat, was then presented with a loud noise (startle response).
Operant conditioning: • Desired behaviors are reinforced (positive, negative), whereas undesirable behaviors are extinguished (punishment).
Modeling (Albert Bandura) • We learn how to behavior, by watching others. • Whether we will produce a given behavior is determined by whether we have seen it reinforced or punished.(Famous Bobo Doll study)
Behavioral therapies • Systematic desensitization (phobias, anxiety) • Flooding (phobias, anxiety) • Aversion conditioning (pedophiles)
Criticisms of theory: • 1. Abnormal behavior not connected to particular learning experiences (schizophrenia). • 2. Simplistic circular reasoning (Description as explanation). • 3. Useful for treatment, but not as cause for most mental disorders.
Cognitive: • Premise- how we organize and interpret information • Criticism of Cognitive Paradigm • Concepts are slippery, not well defined. • cognitive explanations do not explain much • E.g., depressed person has negative cognition--I am worthless.
Therapy • Cognitive-Behavioral therapy • Rational Emotive therapy
E. Humanistic: • Theorists argue we are driven to self-actualize, that is, to fulfill our potential for goodness and growth.
Roger’s Humanistic therapy • We all have a basic need to receive positive regard from the important people in our lives (parents). • Those who receive unconditional positive regard early in life are likely to develop unconditional self-regard. • That is, they come to recognize their worth as persons, even while recognizing that they are not perfect. Such people are in good shape to actualize their positive potential.