Download
1 / 75
750 likes | 759 Vues
Primary angioplasty in patient with shock. HF is the single largest expense for Medicare – > 7 million hospital days/yr for acute HF. – Almost all literature focused on Chronic CHF and not Acute Cardiogenic Shock:

E N D
HF is the single largest expense for Medicare • – > 7 million hospital days/yr for acute HF – Almost all literature focused on Chronic CHF and notAcute • Cardiogenic Shock: • Serious disorder, high death rate, but treatable with improved outcomes if aggressive, but a 50% death rate persists • 5-8% of STEMI patient, 2.5% NSTEMI patients • Approximately 40-50,000 cases/year Hunt SA et al. J Am Coll Cardiol. 2001;38:2101 Graves EJ, Kozak LJ. Vital and Health Statistics. 1999;Series 13:1 AHA. Heart Disease and Stroke Statistics—2005 Update. Available at: http://www.americanheart.org/downloadable/heart/1105390918119HDSStats2005Update.pdf Reynolds HR, Hachman JS Circulation. 2008;117:686-697.
In-hospitalMortalityUSIK 1995, USIC 2000,FAST-MIFrance NationalRegistry Shock 90 80 70 60 50 40 30 20 10 0 70 (62-77) NoShock 63 (56-70) Deathat30days (%) 51 (44-59) 8.7 4.2 3.6 (7.5-10.0) (3.4-5.1) (3.0-4.4) 2000 1995 2005 Aissaoui et al. Eur Heart J 2012; 33:2535–2543
In STEMI, cardiogenic shock increases mortality from 10% to 50%. • Prompt recognition of CS is very important in STEMI management. • Only 15% of STEMI with CS have CS at admission. In the rest, CS usually develops within 24 hours of admission. Case fatality rate in STEMI with and without cardiogenic shock.
ESC definition of CS in STEMI Hemodynamic Clinical Sys BP < 90 mm Hg (or > 90 mm Hg only with drugs or IABP) Diuresis < 20 ml/hr. • CI < 2.2 L/min/m2 • PCWP > 18 mm Hg
Once you identify CS in your STEMI patient, try to identify the cause quickly • Causes of cardiogenic shock- • Large LV territory involved • RVMI in IWMI • VSR, a/c MR, FWR • Look for factors worsening CS- • Arrhythmias • Anemia
Always do an echo prior to PPCI • Extent of LV involved • RV involvement in IWMI • VSR- missed unless you specifically look for it • Acute MR- not as “impressive” as chronic MR • FWR- you won’t have time to do an echo • Co-existing large pericardial effusion
Cause identified. Now what? This talk deals primarily with the first cause.
Patient presents to an interventional cardiology hospital with STEMI with CS due to large part of LV involved. What to do? • Immediate primary PCI • First medical stabilisation. Then PCI once stable. • Immediate fibrinolysis with medical stabilisation. Then PCI once stable.
The Shock Trial has Been the Most Important Study For Management Guidelines in Patients with Cardiogenic Shock HochmanetalNEJM1999;341:625
SHOCK trial : Randomized and controlled study Acute Myocardial Infarction <=36hr Shock <=12hr Randomization Emergency Revascularization Initial medical Stabilization IABP/Pharmacological support Possible prior thrombolysis Emergency early PTCA(60%)/CABG(40%)<= 6 hrs IABP/Pharmacological support Thrombolysis unless absolute Contraindication (63%) Delayed revasc.(25%) >54hr • Primary end point : 30-day mortality • Secondary end point : 6 mo. mortality Hochman et al,NEJM 1999;341:625
SHOCK Trial : Mortality among Study Patients Outcome and Subgroup 30-day mortality Total Age<75yr Age>=75yr 6-mo. mortality Total Age<75yr Age>=75yr ERV 46.7(152) 41.4(128) 75.0(24) 50.3(151) 44.9(127) 79.2(24) Medical Therapy 56.0(150) 56.8(118) 53.1(32) 63.1(149) 65.0(117) 56.3(32) Difference -9.3 -15.4 +21.9 -12.8 -20.1 +22.9 Relative risk 0.83 0.73 1.41 0.80 0.70 1.41 P-value 0.11 0.01 0.027 0.003 percent(number in subgroup) Hochman et al ,NEJM 1999;341:625
SHOCK Trial: Subgroup analysis, Age less than 75 65% 66.7% 56% Revasc. 48.4% 45% 41% Med Rx Mortality P=0.02 CI<1.0 P=0.002 CI<1.0 P<0.02 CI<1.0
SHOCK Trial: What to do with Pt.s older than 75 • Total no. of Pt.s older than 75 y.o. = 56 (/302) • The early revascularization groups had worse outcome at: • 30 days (CI >> 1.0) • 6 months( CI >> 1.0) • 12 months, no difference in outcome
What to do with Pt.s older than 75 • SHOCK Registry results is in contrast to the SHOCK Trial findings in this subgroup. • Those older than 75 y.o., selected to undergo ERV had a survival advantage. • Case by case assessment in this population, and not across the board exclusion is called for.
SHOCK trial- the lesson learned- • Direct CAG is better than initial thrombolytic therapy with CAG later. • Proceed for direct CAG- patient should be stabilized in parallel by critical care team. • O2, CPAP, SOS ventilator • Inotropes
Which inotrope? • Dopamine • Noradrenaline • Dobutamine • Levosimendan • Noradrenaline preferred to dopamine for low BP. • Once BP is > 90 mm Hg systolic- dobutamine or levosimendan.
What if patient presents with STEMI with CS to a non-interventional centre? • STEMI without cardiogenic shock- Fibrinolytic is to be given unless primary PCI can be done in a nearby hospital very fast. • STEMI with cardiogenic shock- Primary PCI is much better than fibrinolysis, delay is acceptable. (How much delay- grey zone).
In STEMI with CS, direct admit patients to interventional centre and transfer patients from non-interventional centres have same in hospital mortality (56% Vs. 55%.) • When patient presents with STEMI with CS to non-interventional centre • Immediate transfer to interventional centre and primary PCI- IHM 41 % • Stabilisation and then transfer if/when stable- IHM 53% (p=0.02)
Patient presents to non-interventional centre with STEMI with CS. Patient cannot be shifted to interventional centre due to some reason. What to do? • No fibrinolysis • Fibrinolysis
Fibrinolysis is better than no fibrinolysis even in STEMI with CS. So if no option to shift to primary PCI centre, give fibrinolysis.
Patient with STEMI with cardiogenic shock, PCI to culprit lesion done, should other lesions, if any, be dealt with in the same sitting?
Classical reasons to avoid non-IRA PCI during primary PCI1. Systemic thrombotic state2. Vasoconstriction exaggerates non-culprit lesions • Roe et al- STEMI all types • IRA + non culprit PCI increased death, reinfarction, CABG and shock • Corpus et al- STEMI all types • IRA + non culprit PCI cf IRA PCI alone in STEMI • More reinfarction • More revascularization • More MACE
But in STEMI with CS, non-IRA PCI decreases mortality. • Complete revascularization at time of primary PCI decreases in hospital mortality compared to culprit PCI only in STEMI with CS. P= 0.02 • Complete revasc cf IRA PCI • Less cardiac death (42% vs 15%) • Less MACE (58% vs 25%)
So non culprit lesion may be done at the time of primary PCI in STEMI with cardiogenic shock if • Both the below conditions are satisfied- • Persistent ischemia after PCI of IRA • Critical lesion (90%) or unstable lesion (thrombus/disrupted lesion) • Preferably by a highly experienced interventionalist. • A procedural complication in non culprit vessel will be catastrophic. • Meticulously analyse coronary anatomy and lesion characteristic. • Preferably avoid if calcified, tortuous, bifurcation, LM or saphenous graft.
Patient presents in STEMI with cardiogenic shock. Any change in loading drugs compared to usual STEMI cases? • Yes. Until CAG is done, do not give clopidogrel/prasugrel/ticagrelor (ESC recommendation)
Intra-Aortic BalloonPump Support • Reduces afterload • Augments diastolic perfusion pressure • Improvement in cardiac output and coronary blood flow • No change in myocardial oxygen demand • IABP support was associated with a ↓ in mortality: • NRMI-2 with lysis, from 67% to 49%2 • SHOCK Trial, from 63% to 47% 1HollenbergAnnIntMed1999;131:47-99 2BarronAHJ 2001;141:933
TACTICS • ST elevation MI patients, presenting within 12 hours of Sx, and Cardiogenic shock • 57 Patients were randomized Thrombolytic Therapy alone Thrombolytic Therapy + IABP
TACTICS • The primary endpoint of 6 month mortality was not statistically significant, P=0.3 • Subgroup analysis: For KILLIP classes III and IV, P=0.07
The NEW ENGLAND JOURNAL of MEDICINE OCTOBER4,2012 ESTABLISHED lN1812 VOL. 367 NO.14 Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shocl< Holger Thiele, M.D., Uwe Zeymer, M.D., Franz-josef Neumann, M.D., Miroslaw Ferenc, M.D., Hans-Georg Olbrich, M.D.,jorg Hausleiter, M.D., Gert Richardt, M.D., Marcus Hennersdorf, M.D., Klaus Empen, M.D., Georg Fuernau, M.D., Steffen Desch, M.D., lngo Eitel, M.D., Rainer Hambrecht, M.D., jorg Fuhrmann, M.D., Michael Bohm, M.D., Henning Ebelt, M.D., Steffen Schneider, Ph.D., Gerhard Schuler, M.D., and Karl Werdan, M.D., for the IABP-SHOCK II Trial Investigators*
Is the IABPIndicated inAll Patients with Cardiogenic Shock? Thieleetal.N EnglJMed 2012;367:1287-96
IABPSHOCKII: 1Year Mortality 30-day mortality 6-month mortality 12-month mortality 60% 51.8%IABP 48.7% Control 50% 41.3% 51.4% 49.2% 40% Mortality 39.7% Logrankp=0.94 30% RR1.02 20% 95%CI0.88-1.19 10% 0% 0 30 60 90 120 150 180 210 240 270 300 330 Daysafterrandomization 360 390 420 No.atrisk IABP Control 301 181 171 165 161 159 154 152 149 147 146 144 136 45 299 174 166 165 159 154 154 152 147 147 146 144 140 55 21 29 Thieleetal.Lancet2013
STEMI with cardiogenic shock- should IABP be used? • Use only if patient does not quickly stabilize with drugs (ACC & ESC) • ACC- Class II A • ESC- Class II B
BCIS Study: Early Results Do Not Support Prophylactic Use of IABP MACCE at Discharge p=0.85 16.0% 15.2% N=150 N=151 Elective IABP Not Planned IABP Perera et al. JAMA 2010 Aug 25;304(8):867-74
BCIS-1 Long Term (5 Year Data) Suggest Benefit to IABP Support in High Risk PCI (hazard ratio, 0.66; 95% confidence Interval, 0.44–0.98; P=0.039 PereraDetal.Circulation.2013;127:207-212
What Constitutes “High Risk PCI?” • Patients for whom high-risk interventions • are considered generally have: • severe diffuse coronary artery disease • a single last patent conduit • Significant unprotected left main disease with large territories of myocardial ischemia • Typically have reduced left ventricular • function (ejection fraction <25%–35%) • Comorbidities that make them high risk for • standard coronary artery bypass grafting. • O’Neill, et al. Circulation. • 2012; 126: 1717-1727
IABP in acute myocardial infarction: When does it make sense?: • large myocardial infarction • ongoing (persistent) ischemia despite successful stenting • whether or not complicated by (pre-)shock • In these patients, IABP significantly decreases mortality! • Van Nunen et al, EuroIntervention, september 2014 ( online) • In CRISP-AMI and SHOCK 2, benefit of IABP was obscured by including too many patients in whom no effect could be expected anyway and by inadequate statistical methods 21
CRISP-AMI: 30-daymortality noIABP IABP no IABP IABP pno<IA0.B0P5 IABP noIABP IABP
IsIABP-therapya matterof timing?
IABPsupport:Isittimedependent? In 119 STEMI patients with cardiogenic shock treated with primary PCI, the use of IABP before intervention was associated with a significantly lower incidence of VF, cardiopulmonary arrest, and total catheterization laboratory events compared with no IABP or IABP after intervention Brodieetal,AmJCardiol1999;84:18-23
ImpactofIABP-Timingin CS Clinical outcomesat 30days Schwarzetal.(submittedforpublication)
Dissectingthedatafor(oragainst)IABP • Conclusions • IABP can be safely applied in shock patients undergoing PCI. • Routine use of IABP in CS, which is not due to mechanical complications is no longer recommended. • IABP-assisted PCI is useful in acute patients with severe shock to support complex interventions.
RandomizedTrial TandemHeartvs. IABPinCardiogenicShock 30d Survival p=ns IABP n=14 Tandem Heart n=19 Burkhoff,AHJ2006;152:469.
PROTECT II TrialDesign Patients Requiring Prophylactic Hemodynamic Support During Non-Emergent High Risk PCI on Unprotected LM/Last Patent Conduit and LVEF≤35% OR 3 Vessel Disease and LVEF≤30% R 1:1 IABP + PCI IMPELLA 2.5 + PCI Primary Endpoint = 30-day Composite MAE* rate Follow-up of the Composite MAE* rate at 90 days *Major Adverse Events (MAE) : Death, MI (>3xULN CK-MB or Troponin) , Stroke/TIA, Repeat Revasc, Cardiac or Vascular Operation or Vasc. Operation for limb ischemia, Acute Renal Dysfunction, Increase in Aortic insufficiency, Severe Hypotension, CPR/VT, Angio Failure
PROTECT IIMACCE Per Protocol Population,N=427 Death, Stroke, MI, Repeat revasc. IABP IMPELLA Log ranktest,p=0.042 MACCE=Death,Stroke, MI*,Repeatrevasc.(*Stoneetal, Circulation2001;104:642-647)
Pre-SpecifiedSub-groupAnalysis (PP) PP=PerProtocol 0.0 0.5 1.0 1.5 2.0 Impella better IABP better O’Neill et al, Circulation. 2012;126(14):1717-27
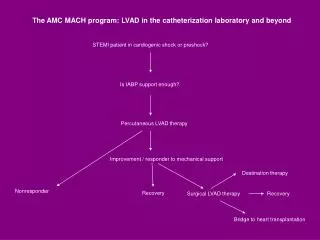
Role of LVAD in STEMI with cardiogenic shock? • Only if there is refractory shock • Class II B (ACC & ESC) • No advantage for LVAD cf. IABP.
Hemodynamic support In patients with cardiogenic shock there is no evidence that routine use of IABP reduces 30 day mortality In patients undergoing high risk PCI, the Impella 2.5, compared to IABP, allows more complete revascularization but does not reduce the incidence of irreversible events A hemodynamic support device is recommended for patients with cardiogenic shock after STEMI who do not quickly stabilize with pharmacologic therapy
What TIMI flow is needed in STEMI with cardiogenic shock? • Always aim for TIMI 3 flow as in any primary PCI • SHOCK trial- STEMI with cardiogenic shock- in hospital mortality • TIMI 3- 26% • TIMI 0/1- 47%